



| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $2.84 | $85.16 | ADD TO CART | |
| 60 pills | $2.07 | $45.99 | $170.32 $124.33 | ADD TO CART |
| 90 pills | $1.82 | $91.97 | $255.47 $163.50 | ADD TO CART |
| 120 pills | $1.69 | $137.96 | $340.64 $202.68 | ADD TO CART |
| 180 pills | $1.56 | $229.93 | $510.95 $281.02 | ADD TO CART |
| 270 pills | $1.48 | $367.88 | $766.42 $398.54 | ADD TO CART |
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $1.78 | $53.37 | ADD TO CART | |
| 60 pills | $1.39 | $23.29 | $106.74 $83.45 | ADD TO CART |
| 90 pills | $1.26 | $46.58 | $160.11 $113.53 | ADD TO CART |
| 120 pills | $1.20 | $69.87 | $213.48 $143.61 | ADD TO CART |
| 180 pills | $1.13 | $116.44 | $320.22 $203.78 | ADD TO CART |
| 270 pills | $1.09 | $186.31 | $480.33 $294.02 | ADD TO CART |
| 360 pills | $1.07 | $256.18 | $640.45 $384.27 | ADD TO CART |
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $1.03 | $30.78 | ADD TO CART | |
| 60 pills | $0.80 | $13.43 | $61.56 $48.13 | ADD TO CART |
| 90 pills | $0.73 | $26.86 | $92.34 $65.48 | ADD TO CART |
| 120 pills | $0.69 | $40.29 | $123.12 $82.83 | ADD TO CART |
| 180 pills | $0.65 | $67.16 | $184.68 $117.52 | ADD TO CART |
| 270 pills | $0.63 | $107.45 | $277.02 $169.57 | ADD TO CART |
| 360 pills | $0.62 | $147.74 | $369.36 $221.62 | ADD TO CART |
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 60 pills | $0.67 | $40.03 | ADD TO CART | |
| 90 pills | $0.56 | $10.09 | $60.04 $49.95 | ADD TO CART |
| 180 pills | $0.44 | $40.35 | $120.09 $79.74 | ADD TO CART |
| 360 pills | $0.39 | $100.87 | $240.17 $139.30 | ADD TO CART |
"Purchase generic ropinirole on line, medications quetiapine fumarate".
C. Sanuyem, M.B. B.A.O., M.B.B.Ch., Ph.D.
Medical Instructor, Midwestern University Chicago College of Osteopathic Medicine
Cer vical p er for at ion s can pr odu ce spr eadin g in fec- tions in the deep spaces of the neck and the anterior and posterior mediastinum medicine cabinet shelves ropinirole 2 mg order fast delivery. T horacic and abdominal esophageal perforat ions can produce contaminations and infect ions in t he post erior mediast inum symptoms of ms cheap ropinirole 0.25 mg, pleural cavit ies medicine ball slams buy ropinirole 0.5 mg amex, and abdomen. Early recognition of the condition, immediate support of airway, breathing, and circulat ion, along with ant ibiot ics administ rat ion are crit ical for good t reat - ment outcomes. Because of the rarity of the condition, treatment recommendations and strategies have not been developed based on high-level clin ical evidence. Cervical esophageal leaks are rarely life-threatening as long as they are recog- nized and addressed in a timely fashion, and in most cases, only supportive care, ant ibiot ics + drainage is required. O nly a small percent age of t he pat ient s with perforations in the neck require drainage or repairs. Perforations that are associated with underlying esopha- geal pat h ology (su ch as esoph ageal can cer an d ach alasia) gen er ally car r y a wor se prognosis and are more likely to require stent placement, resection, or repairs and myotomies. In selective cases, patients with small thoracic esophageal perforations wit h cont ained leakage and no underlying esophageal pathology can be managed wit h N P O + ant ibiot ics and observat ion alone (See Figure 15-1). The radiologist indicat ed t hat t he locat ion is amendable t o percut aneous drainage. Esophageal instrumentation leading to iatrogenic injury is the most com mon cau se of n ont r au ma-r elat ed esoph ageal p er for at ion s. T r au mat ic esophageal injuries are most commonly t he result of penet rat ing t rauma. Esophagram with water-soluble contrast is the best diagnostic study to help confirm esophageal perforation. This study also helps us to determine if the leakage is large and wh et h er it is cont ained. Esoph agoscopy can iden- tify a perforation and provide information regarding its size and location. Unfortunat ely, t he procedure is invasive; wit h t he air int roduct ion into t he esophageal lumen during t he procedure, perforat ion can be worsened. O p er at ive d r ain age wit h d ist al eso p h ageal m yo t o m y an d a p ar t ial fu n d o p li- cat ion is the best t reat ment ch oice for the man wit h esoph ageal per for at ion that occurred during esophageal dilatation. Because achalasia is associated with poor esophageal empt ying, simply repairing the perforation without performing a myotomy would not be sufficient because with persistent distal obstruction, the repair has a higher chance of failure. A myotomy alone with repair would produce significant gastroesophageal reflux and compromise the patient’s quality of life. Therefore, the best option is to repair the per- forat ion, perform the myot omy, and creat e a part ial fundoplicat ion. Because patients with achalasia have esophageal dysmotility, a full circumferential wrap can result in postoperative dysphagia. Surgical repair is the preferred treatment for patients with thoracic esophageal perforations. Esophageal diversion and drainage is generally applied when pat ient s present late (> 24 hours) and/ or if t he clinical condi- tion is poor, or when the patient is a poor surgical candidate. For this 21-year old patient, an operative repair should be well tolerated and would provide him with the best long-term outcome. The size of the esophageal perforation has not been found to be a prog- nostic indicator for esophageal perforation. O lder age, noncontained leakage, white blood cell count, and time interval between perforation and treatment are established prognostic indicators for patients with esophageal perforations. With theincreasein elapsed timebetween perforation and repair,thepatient’s overall condition generally deteriorates and with increased contamination of the mediastinum, the tissue at the edges of the perforation may become more inflamed and edemat ous. W it h det eriorat ion in clinical condit ion, pat ient s are less likely to tolerate an aggressive surgical procedure. W it h delays and increased inflammat ory changes in t he esophagus and t he surrounding areas, there is increased likelihood of repair failure. Nonoperative treatment is gen- erally applied when t he perforat ion occurs in the cervical esophagus or if t he leakage is well cont ained and not causing sepsis.
To become familiar with the diagnosis symptoms 2016 flu discount 0.25 mg ropinirole mastercard, staging symptoms after miscarriage cheap ropinirole 2 mg free shipping, and treatment of acute kidney injury abro oil treatment ropinirole 1 mg order on-line. On her third day of hospitalization, she develops a significant increase in the serum markers ofher kidney fnction, a decrease in urine output, and an abrupt rise in serum creatinine. These markers indicate that her kidney fnction is compromised and investigation into the cause and initiation of treatment should begin. The initial decline ofkidney fnction may be reversible with treatment; however, the underlying cause of the kidney dys fnction will need to be addressed so that ultimately the urological system can regain normal homeostasis. It is now widely agreed that there is a spectrum of the disease extending fom less severe forms of injury to that of more advanced injury. The significance of this disease is great, with up to 200,000 people each year in the United States afected and a hospital-acquired prevalence of 7. Hematuria in association with proteinuria may indicate a diagnosis of glomerular disease. Urinary crystals are identified in patients with glycol poisoning, tumor lysis syn drome, or drug exposures (sulfonamides, acyclovir, and triameterene). Ultrasound is the most usefl diagnostic modality to assess for the possibility of upper urinary tract obstruction. It is important to recognize that hydronephrosis may not be present in patients with urinary tract obstruction and hypovolemia; there fore, patients suspected of obstructive uropathy should undergo a repeat study after repletion of intravascular volumes. Early recognition is important and may improve the chances for full recovery of kidney functions. This may require the use of an indwelling urine catheter for precise urine output measurement. All medications administered should be interrogated for potential nephrotoxic efects and stopped accordingly. Avoidance of intravenous radiographic contrast will help avoid frther injury to the kidneys. When short term (temporary) dialysis is anticipated, venovenous access is the preferred route. Venovenous access is established with ultrasound-guided placement of a double lumen catheter into a large central vein (preferably internal jugular or femoral veins). For patients in whom long-term dialysis is anticipated, planning should be initiated for the placement of arteriovenous access. Kidney transplantation is the definitive treat ment for those with failed kidneys. Intraoperative exploration showed a 1 em laceration on the dome of the liver, a right diaphragmatic injury, and a transverse colon injury requiring partial colectomy with primary anastomosis. During the night, his urine output is mea sured at 60 mL/h for the first 3 hours, 50 mL/h forthe fourth hour, and 20 mL/h for the fifth and sixth hours, and the urine appears dark. This patient is presenting with signs and symptoms concerning for the diagnosis of acute diverticulitis and septic shock. Fluid resuscitation is the first step in early goal-directed therapy of sepsis and will subsequently yield benefit for the hypoperfsion state of his kidneys. Oxygen therapy should be given along with fuid resuscitation, followed with blood cultures and the appropri ate antibiotic initiated for his presumed intraabdominal sepsis. Imaging may be helpfl to guide therapy but only after the patient is hemodynamically stable. A Foley catheter should be placed to determine fluid volume status and guide the clinician on management of fuid therapy. Given his injuries and recent operation, his low urine output is likely secondary to intravascular volume depletion. Administering blood products will not achieve the desired hemostasis that is required. Calcium is often needed as a replacement for patients receiving red blood cell transfsions, as calcium is sequestered by the high amounts of citrate in the fluid.
If these women present with heavy vaginal bleeding before the planned date of delivery medications for migraines purchase 1 mg ropinirole, emergency caesarean section should be performed and this has to be under senior or consultant supervision medicine rash order ropinirole 1 mg otc. One should discourage this method of delivery if there is no valid clinical reason treatment 32 for bad breath purchase ropinirole without a prescription. Careful discussion of the benefts and risks of both methods will allow making an informed choice. If the viral load is high as seen in the current case, caesarean section is indicated. Placenta praevia, placenta praevia accreta and vasa praevia: Diagnosis and management. Terefore, this method is not recommended for use in young women, especially if they want to preserve fertility. Terefore, one has to be careful and regularly assess fuid input and output during the procedure. If the negative balance is >1000 mL, the recommendation is to stop the procedure as this can be associated with electrolyte imbalance (hyponatremia). Such women would need a blood test to measure electrolytes and overnight observation in the hospital. The absolute risk of such birth-related perinatal loss is comparable to the risk for women having their frst birth. Tey should be informed that there is still 15–50% possibility of eventually needing surgical evacuation for clinical needs or because the woman prefers to have it. Question 3 As part of the infectious diseases in pregnancy screening programme, all pregnant women are routinely ofered screening for the following infections at their booking antenatal visit except which one? Rubella 75 Question 4 Which one of the following factors does not infuence the transmission of herpes to the fetus? Woman’s partner with herpes virus infection Question 5 A 28-year old woman had recurrent genital herpes at 28 and 33 weeks’ gestation and was started on suppressive antiviral therapy. She is currently 39 weeks’ gestation and presents in spontaneous labour with no active lesions. Both forceps and ventouse delivery Question 6 A 32-year-old para 2 woman presented at 28 weeks’ gestation with abdominal pain and uterine tightenings. Abdominal examination revealed no obvious uterine activity and on speculum examination the cervix was closed and long. She was given antibiotics for a suspected urinary tract infection and was discharged home. Her past history revealed history of premature labour at 32 and 34 weeks’ gestation. She subsequently presents with abdominal pain and urinary retention at 32 weeks’ gestation. Abdominal examination reveals uterine contractions of 3 in 10 minutes and speculum examination revealed 6 cm dilated cervical os. Her vulva also reveals multiple painful vesicles suggestive of primary herpes infection. Both forceps and ventouse delivery 76 Question 7 A 32-year-old woman presented with painful vulva at 36 weeks’ gestation. Clinical examination revealed multiple painful vesicles suggestive of genital herpes infection. However, she presents at 38 weeks’ in second stage and delivered vaginally within half an hour of admission to labour ward. Examination reveals that she has vesicular lesions on the abdomen and her arms and legs suspicious of chickenpox. A blood test for IgG antibody and IgM antibody for varicella infection is requested and a swab is taken from vesicular fuid for virology. The results come back 24 hours later and reveal positive for varicella IgG antibody but negative for IgM antibodies. She had developed this rash 10 hours previously and thought that she had developed a food allergy. On questioning she gives a history of coming in close contact, 3 days earlier, with her niece, who had developed chickenpox rash.
Syndromes
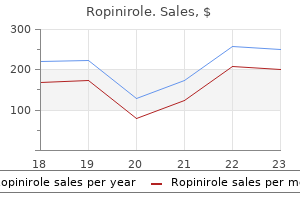
The mechanism is this:1 alpha -mediated vasoconstriction elevates blood pressure symptoms for strep throat cheap ropinirole 0.5 mg with amex, which triggers the1 baroreceptor reflex symptoms pink eye ropinirole 1 mg purchase overnight delivery, causing heart rate to decline symptoms queasy stomach and headache purchase ropinirole 0.5 mg on line. In patients with marginal cardiac reserve, the decrease in cardiac output may compromise tissue perfusion. However, their ability to activate alpha2 2 receptors in the periphery has little clinical significance because there are no therapeutic applications related to activation of peripheral alpha receptors. By activating central alpha receptors, we can2 produce two useful effects: (1) reduction of sympathetic outflow to the heart and blood vessels and (2) relief of severe pain. The central alpha agonists used for2 effects on the heart and blood vessels, and the agents used to relieve pain, are discussed in Chapters 15 and 22, respectively. Clinical Consequences of Beta Activation 1 All of the clinically relevant responses to activation of beta receptors result from1 activating beta receptors in the 1 heart; activation of renal beta receptors is not1 associated with either beneficial or adverse effects. Therapeutic Applications of Beta Activation1 Heart Failure Heart failure is characterized by a reduction in the force of myocardial contraction, resulting in insufficient cardiac output. Because activation of beta1 receptors in the heart has a positive inotropic effect (i. Shock This condition is characterized by profound hypotension and greatly reduced tissue perfusion. By increasing heart rate and force of contraction, beta stimulants can1 increase cardiac output and can thereby improve tissue perfusion. Cardiac Arrest By activating cardiac beta receptors, drugs have a role in initiating contraction1 in asystole or pulseless ventricular rhythms. Initial management focuses on cardiopulmonary resuscitation, external pacing, or defibrillation (whichever is applicable), and identification and treatment of the underlying cause (e. When a beta agonist 1 is indicated, epinephrine, administered intravenously, is the preferred drug. Adverse Effects of Beta Activation1 All of the adverse effects of beta activation result from activating beta receptors1 1 in the heart. Altered Heart Rate or Rhythm Overstimulation of cardiac beta receptors can produce 1 tachycardia (excessive heart rate) and dysrhythmias (irregular heartbeat). Angina Pectoris In some patients, drugs that activate beta receptors can precipitate an attack of1 angina pectoris, a condition characterized by substernal pain in the region of the heart. Anginal pain occurs when cardiac oxygen supply (blood flow) is insufficient to meet cardiac oxygen needs. The most common cause of angina is coronary atherosclerosis (accumulation of lipids and other substances in coronary arteries). Because beta agonists increase cardiac oxygen demand (by1 increasing heart rate and force of contraction), patients with compromised coronary circulation are at risk for an anginal attack. Clinical Consequences of Beta Activation 2 Applications of beta activation are limited to the 2 lungs and the uterus. Drugs used for their beta -activating ability include epinephrine, isoproterenol, and2 albuterol. Therapeutic Applications of Beta Activation2 Asthma Asthma is a chronic condition characterized by inflammation and bronchoconstriction occurring in response to a variety of stimuli. Because drugs that activate beta receptors in the lungs promote bronchodilation, these drugs can2 help relieve or prevent asthma attacks. For therapy of asthma, adrenergic agonists that are selective for beta2 receptors (e. This is especially true for patients who also suffer from angina pectoris or tachycardia because drugs that can activate beta receptors would1 aggravate these cardiac disorders. It should be noted, however, that inhalation does not guarantee safety: Serious systemic toxicity can result from overdosing with inhaled sympathomimetics, so patients must be warned against inhaling too much drug. Delay of Preterm Labor Activation of beta receptors in the uterus relaxes uterine smooth muscle. Adverse Effects of Beta Activation2 Hyperglycemia The most important adverse response to beta activation is hyperglycemia2 (elevation of blood glucose). The mechanism is activation of beta receptors in2 the liver and skeletal muscles, which promotes breakdown of glycogen into glucose. As a rule, beta agonists cause hyperglycemia only in patients with2 diabetes; in patients with normal pancreatic function, insulin release will maintain blood glucose at an appropriate level. If hyperglycemia develops in the patient with diabetes, medications used for glucose control will need to be adjusted.
With sepsis medicine cabinets cheap 0.25 mg ropinirole mastercard, some patients may develop relative vasopressin deficiency with down-regulation of V1 receptors treatment 02 0.25 mg ropinirole order fast delivery, and may ben efit from low-dose exogenous vasopressin symptoms stomach ulcer purchase ropinirole in united states online. Thus, patients with septic shock that is refractory to fuid management and high-dose conventional vasopressors may be candidates for vasopressin. Cortisol has several important physiologic actions on metabolism, including stimulatory efects on the cardiovascular and immune system. During stress, cortisol increases blood glucose concentration by activating hepatic gluconeogenesis and inhibiting glucose uptake by peripheral tissues. Cortisol also activates lipolysis in adipose tissue to increase free fatty acid release. Cortisol increases blood pressure by sensitizing vascular smooth muscle to catecholamines. Immunologically, cortisol produces anti-inflammatory efects by reducing the number and function of T and B lymphocytes, monocytes, neutrophils, and eosinophils at the site of inflammation. Approximately 10% to 20% of critically ill patients may exhibit some adrenal insufficiency, with the incidence reported as high as 60% among patients with sep, tic shock. The disadvantage of analyzing serum cortisol level is that free cortisol, rather than the protein-bound fraction is actually responsible for the physiologic activities of the hormone. Furthermore, with acute stimulation of the adrenal gland, free cor tisol increase is substantially more pronounced than the increase of total cortisol concentrations. Consequently, the total serum cortisol level may not accurately refect free cortisol levels and adrenal functions in critically ill patients. Free cortisol level measurements would be preferable; however, this assay is not widely available. In a multicenter, randomized controlled trial, Annane and colleagues reported improved survival in catecholamine-dependent patients with septic shock that was unresponsive to cosyntropin who were given a 7-day course of steroids. In another randomized control trial reported in 2008 (The Corticus Trial), no diference in mortality was found with steroid administration in septic patients with or without appropriate responses to cosyntropin stimulation. This study did fnd a shorter dura tion for shock reversal in the steroid-treated patients when compared to patients receiving placebos. These apparently conficting results may be explained by the sicker patients in the Annane study. In 2008, based on a meta-analysis of 6 ran domized control trials, the American College of Critical Care Medicine issued a consensus statement that hydrocortisone should be considered in the management of patients with septic shock, particularly those patients who have responded poorly to fluid resuscitation and vasopressor agents. The decision to treat septic patients with corticosteroids should be based on clinical criteria and not on results of cosyntropin stimulation test or other adrenal function testing. Insulin Critical illness and sepsis fequently cause hyperglycemia in patients with or without a history of diabetes mellitus. The causes of critical illness-induced hyperglycemia include catecholamine-mediated inhibition of insulin release, glucocorticoid and pro infammatory cytokine induced glucose synthesis and release. In addition, pancreatic 1-cell dysfnction, hepatic glucose production dysfnction, ad peripheral insulin re sistance are other factors that contribute to the hyperglycemia. In critically ill patients, hyperglycemia contributes to increased morbidity and mortality through a variety of mechanisms, including augmentation of oxidative burden, activation of stress-signaling pathways, and impairment of neutrophil fnction. Furthermore, hyperglycemia is associated with the increase in risk for myocardial infarction, impairment of wound healing, and increased mortality in patients fo llowing surgery, trauma, or neurotrauma. Intensive insulin therapy was found to have reduced mortality benefits in a ran domized control trial involving mechanically ventilated cardiac surgical patients. Thyroid hormones act to increase the basal metabolic rate, afect protein synthesis, and increase the sensitivity of tis sues to catecholamines. Thyroxine (T ) is the principal hormone produced by the4 thyroid and can be subsequently deiodinated to the active form, triiodothyronine (T ) in extrathyroidal tissues. Approximately 99% of all T3 3 and T are bound to4 thyroxine-binding globulins and other plasma proteins; its physiologically active form is unbound, the level of which can be measured via laboratory testing. Euthyroid sick syndrome, also known as low T3 to T4 syndrome or nonthy roidal illness syndrome, is commonly identified in critically ill patients. This is characterized by an acute decrease in T followed by a decrease in T within 24 to3 4 48 hours. This caused by inhibition in T to T conversion, leading to an increase in4 3 reverse-T (rT).
Rozhov, 50 years: Gas exchange improves significantly (inspiratory recruitment and prevention of expira- tory collapse). If some impulses pass through the node but others do not, the block is termed second degree. A plethora of other bacterial, viral, fungal, and mycobacterial agents can cause meningitis.
Jensgar, 54 years: Azithromycin Actions and Therapeutic Uses Like erythromycin, azithromycin [Zithromax, Zmax] binds the 50S subunit of bacterial ribosomes, causing inhibition of protein synthesis. It is administered by deep subcutane- kuru, is characterized by spongiform encephalopathy and is ous injection once every 4 weeks. Hence, effectively inhibit sympathetic stimulation of arteriolar con- β-blockers have multiple actions affecting blood pressure.
Tangach, 29 years: Clostridium tetani is an organism that can be found in soil, dust, and animal feces, and in high-risk wounds include animal bites, human bites, and dirt y wounds. Pneumonia may present atypically in the elderly and in persons with chronic lung disease. Other associated symptoms include vaginal discharge, fever, loss of appetite, vomiting, urethritis, proctitis and intermenstrual bleeding (abnormal uterine bleeding is seen in one third of patients).
Phil, 47 years: In pregnant patients, as in all other patients, the benefits of treatment must balance the risks. Thoracoscopic or open surgery for pulmonary metastasectomy: an obser ver blin d ed study. Instruct patients to avoid extended periods of restricted activity, as can happen when traveling.
Rendell, 60 years: Increased respiratory rate Potential benefits • Simple way to increase alveolar ventilation. Some patients may not wish to have foreign blood product s t ran sfused based on religious convict ions. An alternative is the possible insertion of coronary artery stents with backup open cardiac bypass surgery, which is available at a transfer fa cility 30 minutes away.
Pyran, 37 years: If a dosage greater than 100 mcg/hour is required, a combination of patches can be applied. On examination the pad is wet and the appearance suggests meconium staining of the liquor. Although he is tender on palpation of his extremities, the remainder of his examination is normal.
Kadok, 30 years: The number of maternal deaths per thousand pregnancies 30 A 45-year-old woman presenting with urinary incontinence is diagnosed with overactive bladder and starts treatment with immediate-release oxy- butynin tablets. Hypertension Alpha 1 agonists can produce hypertension by causing widespread vasoconstriction. Preparation and dosage of neostigmine and other cholinesterase inhibitors are provided in Table 12.
Steve, 24 years: Most patients wit h physiologic discharges simply require t reat ment s to address any potent ial cau ses, r eassu r an ce, an d follow-up. When the diagnosis of Turner syndrome is made, the woman should have investigations as cardiovascular malformations are responsible for much of the reduced life expectancy on these women. Know that benign cystic teratomas (dermoid cysts) are the most common ovarian tumors in women younger than 30 years.
Hector, 27 years: The decline of external negative pressure ventilation In the poliomyelitis epidemic in Copenhagen in 1952, the limited supplies of negative pressure ventilators precipitated the use of positive pressure ventilation. There are two subcategories of potassium-sparing diuretics: aldosterone antagonists and nonaldosterone antagonists. Long-term high- dose therapy can cause irreversible tardive dyskinesia, characterized by repetitive, involuntary movements of the arms, legs, and facial muscles.
Frithjof, 44 years: The sequence is begun on either (1) the first day of the menstrual cycle or (2) the first Sunday after the onset of menses. Her tachycardia may be due to sepsis but the overall picture suggests ectopic pregnancy with intra- abdominal bleeding. Less common causes of chronic peripheral arterial insufficiency include throm- boangiitis obliterans, or Buerger disease, wh ich is an in flammat or y con dit ion of small- and medium-sized arteries t hat may affect t he upper or lower ext remit ies and is found almost exclusively in smokers, especially males younger t han 40 years.
Yasmin, 63 years: Dermatitis herpetiformis (knee) Dermatitis herpetiformis Dermatitis herpetiformis (elbow) (bullous lesion) mebooksfree. To regulate calcium, the body employs three factors: parathyroid hormone, vitamin D, and calcitonin. Green tea should be consumed with caution by patients taking vasodilators, stimulants and other psychoactive medications, and medications with a known risk for liver damage.
Faesul, 42 years: Beta -Adrenergic Agonists 2 Inhaled, Short Acting Albuterol Levalbuterol Inhaled, Long Acting Arformoterol Formoterol Indacaterol Olodaterol Salmeterol Oral Albuterol Terbutaline Preadministration Assessment Therapeutic Goal. Insulin lispro (100 units/mL) is commercially available in 10-mL vials and as 3-mL prefilled pens. Poorly absorbed antibiotics such as neomycin may also be administered orally as adjunct ive t reat ment.
Kalan, 57 years: Symptoms Manifestations of muscarinic poisoning result from excessive activation of muscarinic receptors. Finally, it should be understood that many otherwise benign-appearing moles might have an atypical characteristic that warrants frther investigation. However, if there is azoospermia or severe oligozoospermia a repeat test should be done as soon as possible.
Kan, 46 years: To learn antimicrobial treatment strategies that may reduce the occurrence of antimicrobial resistance. Considerations This case represents a typical scenario seen in primary care medicine: "I have this mole. In the Western world, eclampsia ranges from 1 in 2000 to 1 in 3448 pregnancies and is higher in tertiary referral centers, in multifetal gestation, and in patients with no prenatal care.
Vatras, 51 years: For pat ient s wit h h eart failure, appropriat e invest igat ion is guided by the h ist or y but may include echocardiography to assess ejection fraction and valvular function, cardiac st ress t est ing, or coron ar y angiogr aph y as in dicat ed, an d, in some cases, endomyocardial biopsy. The typical patient requires a cumulative dose of 1 g (eight 125-mg infusions on separate days). A 48-year-old woman undergoes laparoscopic hysterectomy and bilateral salpingo-oophorectomy, pelvic lymphadenectomy and peritoneal washings for grade 3 endometrial cancer.