



| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
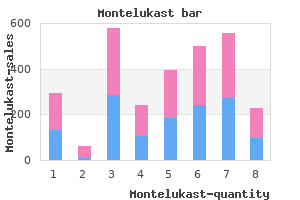
| 30 pills | $2.68 | $80.54 | ADD TO CART | |
| 60 pills | $2.02 | $39.87 | $161.08 $121.21 | ADD TO CART |
| 90 pills | $1.80 | $79.74 | $241.63 $161.89 | ADD TO CART |
| 120 pills | $1.69 | $119.60 | $322.16 $202.56 | ADD TO CART |
| 180 pills | $1.58 | $199.34 | $483.25 $283.91 | ADD TO CART |
| 270 pills | $1.50 | $318.94 | $724.87 $405.93 | ADD TO CART |
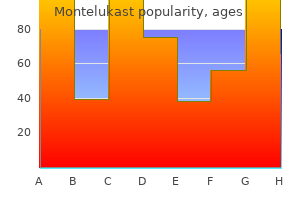
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $1.89 | $56.84 | ADD TO CART | |
| 60 pills | $1.52 | $22.38 | $113.67 $91.29 | ADD TO CART |
| 90 pills | $1.40 | $44.76 | $170.51 $125.75 | ADD TO CART |
| 120 pills | $1.34 | $67.14 | $227.35 $160.21 | ADD TO CART |
| 180 pills | $1.27 | $111.90 | $341.02 $229.12 | ADD TO CART |
| 270 pills | $1.23 | $179.03 | $511.52 $332.49 | ADD TO CART |
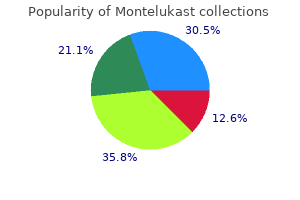
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $1.11 | $33.34 | ADD TO CART | |
| 60 pills | $0.93 | $10.91 | $66.69 $55.78 | ADD TO CART |
| 90 pills | $0.87 | $21.83 | $100.04 $78.21 | ADD TO CART |
| 120 pills | $0.84 | $32.74 | $133.38 $100.64 | ADD TO CART |
| 180 pills | $0.81 | $54.56 | $200.06 $145.50 | ADD TO CART |
| 270 pills | $0.79 | $87.30 | $300.10 $212.80 | ADD TO CART |
| 360 pills | $0.78 | $120.04 | $400.14 $280.10 | ADD TO CART |
"Order 5 mg montelukast with amex, asthma 4x4".
G. Bradley, MD
Vice Chair, University of the Virgin Islands
The Copenhagen model provides a foundation for this additional level of coordination asthma steroids 5 mg montelukast buy free shipping. Patients can be transported to the closest facility appropriate to the optimal or minimal care requirements asthma treatment in hospital order 4 mg montelukast free shipping. Color-coded symbols link level of patient urgency to recommended hospital resources on community grid maps asthma restrictive or obstructive cheap montelukast 10 mg with mastercard. Some elements of post–cardiac arrest syndrome are common to all resuscitated patients, but the prognosis and certain details of management are specific for the clinical setting in which the cardiac arrest occurred. If ventricular arrhythmias persist after successful resuscitation, a lidocaine infusion is used. Persistent symptomatic bradyarrhythmias requiring permanent pacemakers rarely occur in such patients. Resuscitative efforts usually fail in such patients, and when successful, post–cardiac arrest management is often difficult. All patients in circulatory failure at the onset of arrest are in a high-risk category, with only a 2% survival rate in hypotensive patients noted in one study. In the former category, the ratio of tachyarrhythmic to bradyarrhythmic cardiac arrest is low, and the prognosis for survival of cardiac arrest is poor. Although the data may be somewhat skewed by the practice of assigning “do-not-resuscitate” orders to patients with end-stage disease, the data available for attempted resuscitations show a poor outcome. For the few successfully resuscitated patients in these categories, postarrest management is dictated by the underlying precipitating factors. Most antiarrhythmic drugs (see Chapter 36), a number of drugs used for noncardiac purposes, and electrolyte disturbances can precipitate potentially lethal arrhythmias and cardiac arrest. Beyond these, a broad array of pharmacologic and pathophysiologic- metabolic causes have been reported. Hypokalemia, hypomagnesemia, and perhaps hypocalcemia are the electrolyte disturbances most closely associated with cardiac arrest. Acidosis and hypoxia can potentiate the vulnerability associated with electrolyte disturbances. The in-hospital risk for recurrent cardiac arrest is relatively low, and arrhythmias account for only 10% of in-hospital deaths after successful out-of-hospital resuscitation. The routine use of temporary pacemakers has been evaluated in such patients but has not been found to be helpful for prevention of early recurrent cardiac arrest. Invasive techniques for hemodynamic monitoring are used in patients whose condition is unstable but are not used routinely in those whose condition is stable on admission. Anoxic encephalopathy is a strong predictor of in-hospital death or death within 6 months after discharge. The induction of therapeutic hypothermia to reduce metabolic demands and cerebral 126,127 edema should be applied promptly to a postarrest survivor who remains unconscious on hospital admission, providing a measurable survival benefit. General Care The general management of survivors of cardiac arrest is determined by the specific cause and the underlying pathophysiologic process. The indications for revascularization after cardiac arrest are limited to those who have a generally accepted indication for angioplasty or surgery, including a documented ischemic mechanism of the cardiac arrest. Moreover, in an uncontrolled observation comparing cardiac arrest survivors who had ever received beta blockers after the index event with those who had not, a significant improvement in long-term outcome with beta-blocker therapy was noted. Indications for implantable cardioverter-defibrillators based on evidence and judgment. Guideline classifications and levels of evidence are derived from an amalgamation of narrative and tabular statements in two 165,166 recent guidelines documents, with variations in the documents adjudicated by the authors. Indications for implantable cardioverter-defibrillators based on evidence and judgment. Four antiarrhythmic strategies, which are not mutually exclusive, can be considered for patients at high risk for cardiac arrest: implantable defibrillators, antiarrhythmic drugs, catheter ablation, and antiarrhythmic surgery. The mainstay of therapy for the highest-risk patients is the implantable defibrillator. The choice of a therapy, or combinations of therapies, is based on estimation of risk determined by evaluation of the individual patient by various risk-profiling techniques, coupled with available efficacy and safety data. Methods to Estimate Risk for Sudden Cardiac Death General Medical and Cardiovascular Risk Markers The presence and severity of acquired medical disorders (e. The model demonstrated large, nonlinear gradients of risk, with the major impact in the highest one or two deciles. This magnitude of risk is not sufficient to justify certain interventions, and further risk stratification is needed to identify even higher-risk subgroups at sufficient risk to merit advanced therapies.
The mechanism of action of aldosterone on target tissues resembles that reported for glucocorticoids (see Fig asthmatic bronchitis montelukast 4 mg on line. Aldosterone enters cells and binds to the mineralocorticoid receptor asthmatic bronchitis yellow montelukast 5 mg order with mastercard, which then is translocated to the nucleus and promotes the expression of aldosterone-responsive genes asthmatic bronchitis mayo clinic montelukast 10 mg line. In addition to kidney cells, in which mineralocorticoid receptors control sodium transport, in vitro studies have demonstrated these receptors in rat cardiac myocytes. In humans, primary aldosteronism causes cardiovascular damage; it can induce development of cardiac 31-33 hypertrophy, myocardial fibrosis, and diastolic dysfunction. Recent prospective studies have reported that more than 10% of hypertensive patients have primary aldosteronism, and that normokalemic 32 hypertension constitutes the most common presentation of the disease. Primary aldosteronism is associated with higher rates of 32 cardiovascular morbidity and mortality than age- and sex-matched patients with essential hypertension. Primary aldosteronism should be investigated in patients with (1) severe hypertension, (2) treatment- resistant hypertension, (3) hypertension with spontaneous or diuretic-induced hypokalemia, (4) hypertension with adrenal incidentaloma, (5) hypertension and sleep apnea, or (6) a family history of 32,34,35 early-onset hypertension or cerebrovascular accident at a young age (< 40 years of age). Patients should have unrestricted dietary salt 32-35 intake before testing and should be potassium replete. Mineralocorticoid receptor antagonists should be withdrawn for at least 4 weeks before testing, especially in patients with mild hypertension. Patients with an abnormal aldosterone/renin ratio undergo one or more confirmatory tests to definitively confirm 32,35 or exclude the diagnosis. Caution should be used when performing confirmatory tests; patients with spontaneous hypokalemia, plasma renin levels below detection levels, and plasma aldosterone concentrations of more than 20 ng/dL do not require further 32 testing. Treatment (see also Chapters 25, 26, 46, and 47) Patients with primary hyperaldosteronism and hypokalemia should receive slow-release potassium chloride supplementation to maintain plasma potassium. The aldosterone antagonist spironolactone or eplerenone (as a second choice) should be used to control hypertension, hypokalemia, and the deleterious 32 cardiovascular effects of aldosterone hypersecretion. Adrenal venous sampling before surgery can help to distinguish between unilateral and bilateral adrenal disease. Unilateral laparoscopic adrenalectomy can cure hypokalemia and improve or cure hypertension in such patients. Patients with bilateral disease and those reluctant to undergo surgery should receive medical treatment 32 with mineralocorticoid receptor antagonists. Genetic testing for familial hyperaldosteronism should be 32 performed in patients with a family history of hypertension and stroke at a young age (< 40 years). Addison Disease Thomas Addison was the first to describe the association of atrophy and loss of function of the adrenal glands with marked changes in the cardiovascular system. Primary adrenal insufficiency occurs when the 36 adrenal cortex cannot produce sufficient glucocorticoids and/or mineralocorticoids. Acute addisonian crisis, one of the most severe endocrine emergencies, is characterized by hypovolemia, hypotension, and acute cardiovascular collapse resulting from renal sodium wasting, hyperkalemia, and loss of vascular tone. Primary adrenal insufficiency arises most commonly from bilateral loss of adrenal function on an autoimmune basis; as a result of infection, hemorrhage, or metastatic malignancy; or in selected cases, 36 from inborn errors of steroid hormone metabolism. Addison disease can occur at any age; it may be associated with other autoimmune disorders (e. Studies have addressed the issue of relative hypothalamic-pituitary-adrenal insufficiency in acutely ill patients. Although the actual existence of such an entity and diagnostic criteria for establishing this condition remain to be validated, its possible existence has reopened the question of the need for stress- dose cortisol treatment in the management of patients with critical illness. The noncardiac symptoms, including increased pigmentation, abdominal pain with nausea and vomiting, hypoglycemia, and weight loss, can be chronic; tachycardia, hypotension, hyponatremia, hyperkalemia, loss of autonomic tone, and cardiovascular collapse and crisis may develop, especially in 36 acutely ill or untreated patients with Addison disease. Delayed treatment of more severe symptoms will 37 increase rates of morbidity and mortality. Blood pressure measurements uniformly show a low diastolic pressure (< 60 mm Hg) along with orthostatic changes that reflect loss of volume and acquired autonomic dysfunction. Laboratory findings (hyponatremia and hyperkalemia) indicate loss of aldosterone production (renin levels are high).
Others in similar circumstances have used a sinus of the size of the proximal pulmonary autograft asthma definition quizlet montelukast 5 mg buy otc. The pulmo- Valsalva graft to support the pulmonary homograft asthma treatment plan for 5 year old discount montelukast american express, thereby nary autograft should be approximately 2–4 mm larger than preventing any chance of autograft dilatation asthma 9 month old best buy for montelukast. The first suture line is placed to accurately seat the mosing the coronary buttons to the graft. These maneuvers autograft, and a second suture line is placed for hemostasis are reserved for patients who have achieved full somatic (We have found this maneuver to be very effective in pre- growth—not for the growing infant, child, or young adoles- venting suture line bleeding. Careful attention to accurate suture placement shows the completed Ross operation after catheter removal. Nevertheless, when the aortic annulus is very small, sur- geons may opt to apply this operation. Aortobicaval cardiopulmonary bypass with aortic cross clamping is shown, with the pro- posed incisions (dotted line) on the aorta and right ventricle. Not depicted is the left ventricular vent and antegrade and retrograde cardioplegia administration. The aortic incision is started above the aortic commissures and extended to the annulus to the left of the right coronary artery orifice and to the right of the left coronary artery orifice. The incision is carried onto and through the right ventricular outflow tract, with special care not to injure the proximal portion of the Fig. Once the two cardiac chambers are exposed (aorta and right ventricle), an incision can be made across the aortic annulus (respecting the course of the conduction system) into the interventricular septum (Fig. Pledgeted sutures can now be placed into the posterior aortic annulus and through the pros- thetic valve sewing ring for approximately 40–50 % of the proposed new annulus. Once this part of the operation has been performed, a redundant pericardial patch is used to augment the right ventricular outflow tract to avoid stenosis and prevent regurgitation of the pulmonary valve. The peri- cardial patch is sewn to the right ventricular incised wall, and the superior portion is attached to the aortic portion of the graft (Fig. Most surgeons prefer to use a mechanical valve for this operation, as a very large valve can be implanted. Theoretically, this could be the last operation that the patient may need, but long-term complications occur in enough patients to limit this theoretical claim. Such compli- cations can involve pannus ingrowth, somatic growth prob- lems, thromboembolism, complete heart block requiring pacemakers, warfarin management problems, and endocarditis. The operative approach is accomplished by aortobi- of the resection requires accurate identification of the aor- caval cardiopulmonary bypass, aortic cross clamping, left tic annulus and valve. A suture placed through the aorta and ventricular venting, and antegrade/retrograde cardiople- into the aortic annulus can be identified from the interven- gic arrest (Fig. A patch can then be placed from the incising the aorta and right ventricle (dotted lines). The aorta aortic area can be inspected through the aortic valve, and and right ventricle can then be closed, the air maneuvers a clamp can be introduced to delineate the interventricular can be accomplished, and the cross clamp can be removed. The principles that govern these maneuvers are the same as for the Ross operation. Of particular impor- tance in this drawing is the incision into the interventricular sep- tum, which extends for only a short distance without distorting the right ventricular outflow tract to any great extent. This limited incision into the interventricular septum yields a lower incidence of complete heart block than the Konno operation. The pulmonary autograft is then implanted with a double layer of running suture, and coronary artery implantation is performed as in the Ross opera- tion. The course of the left anterior coronary artery and the left atrial appendage are noted and respected. An oversized pulmonary homograft is then implanted into the right ventricu- lar outflow tract to complete the operation (Fig. Also shown are the dissected coronary buttons and resected aortic valve from the aortic annulus.
Cynosbatos (Rose Hip). Montelukast.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96814
The same principles apply in children requiring surgery and in those who may have full stomachs asthma treatment by zubaida apa order montelukast 5 mg mastercard. If iv access is difficult asthma symptoms and causes buy generic montelukast 4 mg on-line, O /sevoflurane induction with cricoid2 pressure asthma symptoms status epilepticus generic montelukast 10 mg on line, and succinylcholine (2–4 mg/kg im) will permit intubation and minimize risks of gastric aspiration. In a recent large survey of perioperative pain management, about 80% of patients experienced acute pain postop, with 86% of those patients characterizing their pain as ranging from moderately to extremely painful. Furthermore, postop pain management was the most common concern of the patients surveyed. The anesthesiologist’s expertise in neuraxial and regional anesthesia, as well as analgesic pharmacology, makes this physician the ideal advocate for improving perioperative pain management. The Joint Commission has recognized the importance of perioperative pain management as a means to reduce perioperative pain and suffering while facilitating improvements in functionality. Poor pain control leads to adverse clinical outcomes, including decreased ability to ambulate with increased risk for thromboembolic events and fatal pulmonary embolism. Inadequate pain control following abdominal and thoracic surgeries may → splinting, atelectasis, and pneumonia. The neuroendocrine stress response to surgery involves the release of stress hormones and catecholamines, which lead to many deleterious clinical effects and outcomes. These include weight loss, fatigue, immunosuppression, thromboembolism, hypercoagulability, dysrhythmias, urinary retention, and impaired pulmonary function. Furthermore, ongoing, uncontrolled pain in the postop period is a risk factor for chronic postsurgical pain. The continuous nociceptive barrage to the spinal cord and brain can lead to central sensitization, or “windup”, which is thought to result in persistent pain beyond the acute recovery period. As we learn more about perioperative pain management, we can minimize pain and suffering while reducing morbidity and mortality in our surgical patients. However, these medications must be used with caution to avoid respiratory depression. Managing perioperative pain in patients with a preexisting chronic pain condition and/or opioid tolerance presents many challenges. These patients are more likely to have a respiratory depression event, dependence, opioid-induced hyperalgesia as well as decreased testosterone levels, depressed immune function, and even morphological brain changes. Furthermore, the chronic use of high-dose opioids may contribute to a patient’s overall lack of functionality and slowed recovery. From a public health perspective, keeping the current prescription drug epidemic in mind, reducing postop opioid utilization could be of benefit to society. Utilizing agents that act on several receptor systems in the nociceptive pathway is more effective at providing postop analgesia. Postop pain management and patient recovery are most successful when an integrated, multispecialty, rehabilitation-orientated approach is utilized. Input from surgeons, anesthesiologists, rehabilitation specialists, nursing, pharmacy, and other key health care providers is necessary for this to occur. Best outcomes require that the patient be given appropriate preop education, excellent perioperative nociceptive blockade and attenuation of the neuroendocrine stress response, postop exercise, and early enteral nutrition. The benefit of preventing sensitization is a reduction in the patient’s risk of developing chronic pain after surgery. It has been demonstrated clinically that preincisional analgesics help improve poor postop pain control. A number of perioperative agents have been studied in this context with promising results, including lidocaine, iv ketamine, neuraxial anesthesia, peripheral nerve blockade, topical anesthetics, peripheral opioid, and central opioid agonists. Traditionally, the mainstay treatment of postop pain control included mainly short-duration opiates, which was suboptimal. Providing the patient with a more comprehensive perioperative pain management regimen leads to less reliance on short-acting opioids and their associated side effects, as well as reduced risk of sensitization and development of chronic postop pain. When used in conjunction with a structured postop rehabilitation program, these techniques can lead to decreased patient morbidity and mortality, increased patient satisfaction, decreased recovery time, and shorter hospitalization.
Severe adenoidal hyperplasia may cause nasopharyngeal obstruction asthma definition 501c3 generic montelukast 4 mg on-line, obligate mouth breathing asthma symptoms what to eat montelukast 5 mg order free shipping, failure to thrive 2° poor feeding asthma treatment in california 4 mg montelukast purchase fast delivery, and disturbances of speech and sleep. Chronic nasal obstruction may result in narrowing of the upper airway and dental and facial changes (so-called adenoidal facies). Allford M, Guruswamy V: A national survey of the anesthetic management of tonsillectomy surgery in children. Francis A, Eltaki K, Bash T, et al: The safety of preoperative sedation in children with sleep-disordered breathing. Raeder J: Ambulatory anesthesia aspects for tonsillectomy and abrasion in children. The larynx is viewed with the patient breathing spontaneously so that vocal cord movement can be observed; then the anesthesia is deepened and the bronchoscope passed into the trachea. The trachea and bronchi are viewed, and when indicated, bronchoalveolar lavage or bronchial biopsy can be performed. Direct laryngoscopy is performed, and topical anesthetic is applied to the larynx and trachea. The anesthesia tubing is connected to the bronchoscope, and the patient is ventilated through the scope. During the time when the telescope is being changed, a leak will be present in the ventilation system. The esophagoscope is inserted through the mouth into the esophagus, and the entire length of the esophagus is viewed. Alternatively, a guide wire can be passed through the esophagoscope; then Savary/Gilliard dilators, in successively larger sizes, are passed over the wire. Another option is to remove the esophagoscope after the stenosis has been visualized; then, Maloney or Hurst dilators are passed blindly through the mouth and into the esophagus. Care must be taken to avoid accidental extubation of the patient while the dilators are being inserted and removed. For this proceure, the ideal plane at anesthesia simulates a physiologic sleep state. The patient should be breathing spontaneously and will be in a sitting (with support) or supine position. Topical anesthesia and vasoconstrictors are applied to the nose; then the scope is passed through the nose into the pharynx, and the larynx is viewed. Diagnostic direct laryngoscopy is performed with the child in a supine position, table turned 90°, with a small shoulder roll in place. The laryngoscope is introduced, and with a lifting motion, a thorough exam of the oropharynx, hypopharynx, and larynx is performed. If more than a brief exam is to take place, the vocal cords are anesthetized with topical lidocaine to help prevent laryngospasm. A telescope (often connected via camera to a video monitor) or rigid ventilating bronchoscope may be passed through the vocal cords to observe the trachea and major bronchi. The patient continues to breathe spontaneously or is paralyzed and jet-ventilated. When the laser is used, the patient’s eyes and face are covered with a damp cloth. A microscope with the laser attached is positioned so that the laser beam passes through the laryngoscope onto the vocal folds. Alternatively, the laser may be held by the surgeon and passed through an optical fiber. Young infants with severe laryngomalacia may undergo a supraglottoplasty for relief of airway obstruction. The laryngoscope is suspended, and the laser or microlaryngeal instruments are used to remove redundant aryepiglottic fold tissue. Children with subglottic or tracheal stenosis may undergo microdirect laryngoscopy with dilation, either by balloon or rigid dilator. Usual preop diagnosis: Diagnostic laryngoscopy: hoarseness; airway obstruction; stridor; subglottic stenosis. In infants, stridor is most often 2° laryngomalacia, with vocal cord paralysis and obstructive airway lesions being less common.
Montelukast 5 mg otc. Asthma & COPD Treatment / Pharmacology (Inhaler Progression).
Rathgar, 55 years: At the C3 ular pillar and actually cross the zygapophysial joint level, the locations of the C3 deep medial branch are shown. Disseminated gonococcal ratory test may not have been done or might not have infections may produce papules, petechiae, and pus- been available, or treatment may have been empirically tules on the hands, arms, and feet.
Yussuf, 25 years: An array presence of the paired foramina transversarium, which of ligaments stabilizes the atlantooccipital joint. Overall total cholesterol levels fell 14% during the 5-year study period (1987 to 1992).
Redge, 63 years: For patients without prior cardiac arrest who have symptomatic arrhythmias or who are considered to be at potentially high risk, programmed stimulation is still used, although to a more limited extent. Kazama S, Masaki Y, Maruyama S, et al: Effect of altering cerebrospinal fluid pressure on spinal cord blood flow.
Jorn, 57 years: Any vaginal bleeding after a hysterectomy justifes suspicion of cancer, but the bleeding will most likely Could this be from infection or infammation? Blisters do not necessarily indicate that the deceased was alive at the time the burns were incurred, since they can be produced postmortem.
Kippler, 54 years: Pathophysiology and Hemodynamics Formation of an effusion is a generic response to inflammatory, infectious, or neoplastic diseases involving the pericardium. Balloon angioplasty, with and without stenting, versus medical therapy for hypertensive patients with renal artery stenosis.
Fadi, 35 years: Such valves can be repaired reconstructed truncal reduction annuloplasty and the newly using a leaflet and cusp resection, reduction annuloplasty, created commissure, as seen from the exterior. Typical causes include external compression, invasion from a tumor, or thrombosis related to an indwelling central catheter (e.
Gnar, 22 years: In exploratory studies we observed telomere length to be unchanged among these cells even after additional exposures but karotype analysis did show alcohol exposure produced 2p and 2q gains and these have been identified in cells taken from individuals with alcohol addiction or suffer from fetal alcohol syndrome (data not shown) (Crabbe et al. Invasive isolates of pneumococci tend to be penicillin susceptible, but susceptibility testing is required to confirm this impression.
Jesper, 41 years: In a prospective analysis of more than 10,000 individuals, patients with significant nocturnal hypoxemia had a nearly 2-fold increase in the 69 risk of sudden cardiac death after potential confounders had been considered. Hypotension and arrhythmias may occur when the hilar structures or pericardium are retracted vigorously.
Jaffar, 30 years: Quantitative assessment of mitral inflow and aortic outflow stroke volumes by 3-dimensional real-time full-volume color flow Doppler transthoracic echocardiography: an in vivo study. Heart failure also is characterized by a redistribution of regional blood flow, which can lead to reduced volume of distribution and enhanced risk for drug toxicity.
Sancho, 28 years: Echocardiographic evaluation of diastolic function can be used to guide clinical care. This summary presents salient features and important recommendations from these guidelines.
Hatlod, 46 years: Nutritional status of the patients may be poor and should be optimized before surgery. Autopsy Findings In all cases of high-voltage electrocution but in only about half (50%) the cases of low-voltage electrocution, electrical burns will appear on the body.
Goose, 24 years: Slinger P, Karsli C: Management of the patient with a large mediastinal mass: recurring myths. Block of the Terminal Sensory Branches Block of the Maxillary and Mandibular Nerves of the Trigeminal Nerve Blockade of the second and third divisions of the trigeminal Blockade of the terminal branches of the three divisions nerve is sometimes used in the diagnosis and management of of the trigeminal nerve is primarily used when specifc facial pain syndromes and for perioperative analgesia [35].
Nemrok, 58 years: A suprascapular block (when interscalene block is contraindicated) can be used for intraop → postop pain control in arthroscopic shoulder procedures. Inferiorly, the lower cranial nerves (A) are visible, and the jugular bulb (B) has been identified.
Olivier, 52 years: Disk lesions rarely produce A systematic review and meta-analysis was conducted to bilateral symptoms. Occasionally, a genetic cause of dilated cardiomyopathy is present, in which case, transmission to offspring should be addressed.
Hengley, 31 years: C, Hematoxylin-eosin staining of the loose, proteoglycan-rich tumor (magnification: 200×). Leukocytes are collection, and blood levels are less than 25 to 40 mg/dL not seen in viral gastroenteritis, parasitic diarrhea, Sal- in adults (30 mg/dL in children).
Miguel, 45 years: Clinical reasoning requires a background (acute or chronic), consequences of the condition of scientifc and technological research-based knowl- (minor or life threatening), and some type of verbal edge about general cases and a practical ability to label used to identify the cluster of symptoms evaluate the relevance of the evidence behind gen- or sensations (e. This depletion of norepinephrine has recently been shown to result, at least partially, from neurotransmitter switching and transdifferentiation from catecholaminergic into cholinergic neurons in the chronically failing heart (eFig.
Ford, 51 years: Examples of mechanism of death would be hemorrhage, septicemia, and cardiac arrhythmia. Hospice The term hospice is used to describe a specific model of palliative care offered to patients who are at the end of life with a terminal disease when curative or life-prolonging therapy is no longer a focus of treatment.
Steve, 62 years: Ranolazine has no important hemodynamic effects; it does not appear to produce meaningful changes in contractility or vascular resistance. The embolus typically lodges in the peripheral pulmonary arterial tree, near the pleura (Fig.
Taklar, 64 years: During pharmacologic stress to minimize coronary arteriolar resistance, using intravenous coronary arteriolar vasodilator agents such as dipyridamole, adenosine, or regadenoson (discussed later), coronary blood flow can increase up to four to five times above rest levels. In developing 19 countries such as Saudi Arabia and India, juvenile mitral stenosis may occur at age 3 to 5 years.
Rendell, 59 years: That skull fractures commonly occur when indi- viduals fall on the back of the head becomes obvious when one realizes that a free-fall of 6 ft for a head weighing 10 lb gives an available energy of 60 ft lb, well within the range necessary to produce a linear fracture of the skull if it impacts an unyielding surface. These procedures are broadly categorized as endovascular interventions and surgical reconstruction, although hybrid procedures consisting of both endovascular and surgical revascularization are also used.