



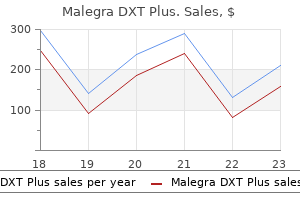
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 20 pills | $1.90 | $37.94 | ADD TO CART | |
| 30 pills | $1.60 | $9.01 | $56.90 $47.89 | ADD TO CART |
| 60 pills | $1.30 | $36.06 | $113.82 $77.76 | ADD TO CART |
| 90 pills | $1.20 | $63.10 | $170.73 $107.63 | ADD TO CART |
| 120 pills | $1.15 | $90.14 | $227.63 $137.49 | ADD TO CART |
| 180 pills | $1.10 | $144.23 | $341.45 $197.22 | ADD TO CART |
| 270 pills | $1.06 | $225.36 | $512.18 $286.82 | ADD TO CART |
"Buy malegra dxt plus 160 mg otc, impotence essential oils".
G. Phil, MD
Medical Instructor, Medical College of Wisconsin
Understand that the most common cause of uterine inversion is undue trac- tion of the cord before placental separation erectile dysfunction doctor omaha cheap malegra dxt plus 160 mg buy online. Co n s i d e r a t i o n s This patient’s history reveals that the first and second stages of labor are normal erectile dysfunction doctors raleigh nc purchase generic malegra dxt plus canada. The third stage of labor (placental delivery) reaches close to the upper limits of normal erectile dysfunction otc purchase 160 mg malegra dxt plus mastercard. There is evidence for partial placental separation, but there were not clear sign s of complete placent al separation such as lengthening of the cord. The four sign s of placent al separat ion are (1) gu sh of blood, (2) lengt h en ing of the cor d, (3) globular and firm sh ape of the ut erus, and (4) the ut er us rises up t o the anterior abdominal wall. In this case, although there is not good evidence for placental separation, traction on the cord is exerted, which results in an inverted uterus. The reddish bulging mass noted adjacent to the placenta is the endometrial surface; hence, the mass will have a shaggy appearance and be all around t he pla- cent a. O t h er masses an d/ or or gan s may at t imes pr olapse, su ch as vagin al or cer vi- cal t issu e, but t h ese will h ave a sm oot h app ear an ce. Uterineinversioncanoccurwhenexcessiveumbilicalcordtractionis exerted on a fundally implanted, unseparated placenta (A). Up o n re co g n it io n, the o p e ra t o r at t e m p t s to reposition the inverted uterus using cupped fingers (B). Because the uterus and placenta are no longer joined, the placenta is usually in the lower segment of the uterus, just inside the cervix, and the uterus is often contracted. The umbilical cord lengthens due to the placenta having dropped into the lower portion of the uterus. The gush of blood represents bleeding from the placental bed, usually coinciding with placental separation. If the placenta has not separated, excessive force on the cord may lead to uterine inver- sion. Massive hemorrhage usually result s; t hus, in t his situat ion, t he pract it ioner must be prepared for rapid volume replacement. Although it was classically taught by some that the shock was out of proportion to the actual amount of blood loss, this is not the case. The best method of averting a uterine inversion is to await spontaneous separa- tion of the placenta from the uterus before placing traction on the umbilical cord. Even aft er one or t wo signs of placent al separat ion are present, the operat or sh ould be cautious not to put undue tension on the cord. At times, part of the placenta may separate, revealing the gush of blood, but the remaining attached placenta may induce a uterine inversion or t raumat ic severing of the cord. The grand-mult ipa- rous patient with the placenta implanted in the fundus (top of uterus) is at particu- lar risk for ut erine inversion. If the placenta has already separated, the recently inverted uterus may somet imes be replaced by using the gloved palm and cupped fingers. Two int rave- nous lines should be started as soon as possible and preferably prior to placental separat ion, since profuse hemorrhage may follow placental removal. Terbutaline or magnesium sulfate can also be utilized to relax the uterus if necessary prior to uter- ine replacement. Upon replacing t he ut erine fundus t o t he normal locat ion, the relaxation agents are stopped, and then uterotonic agents, such as oxytocin, are given t o pr event r e-inver sion an d also t o slow d own the bleedin g. P lacem ent of the clin ician’s fist in sid e the ut er u s t o maint ain the n or mal st r u ct u r e of the ut er u s may help to prevent re-inversion. Note: Even with optimal treatment of uterine inversion, hemorrhage is almost a cert aint y. In several studies, active management slightly reduces the incidence of postpartum hemorrhage, probably due to early use of utero- tonic agents (usually after delivery of the baby’s anterior shoulder). Proponents of physiologic management of labor argue that there is less risk of entrapment of a retained placenta (due to difficulty with manual separation when uterotonic agents are given), and less chance of uterine inversion. Upon delivery of the placenta, there was noted to be an inverted uterus, which was successfully managed including replacement of the uterus. Which of the following placental implantation sites would most likely predis- pose to an inverted uterus? Aft er the deliver y, the placent a does n ot deliver even aft er 30 minut es. Delivery of the placenta is complicated by an inverted uterus, with subsequent hemorrhage leading t o 1500 mL of blood loss.
Syndromes
For example erectile dysfunction treatment cost in india malegra dxt plus 160 mg buy without prescription, if the steady-state gentamicin concentration is 2 mg/L and the clearance rate for gentamicin is 100 mL/min (0 impotence from priapism surgery discount malegra dxt plus 160 mg on-line. If the drug is to be administered every 8 hours causes of erectile dysfunction in 60s purchase malegra dxt plus 160 mg without a prescription, then Tmax the dosage would be calculated as follows: Time Maintenance dose = Hourly rate × dosage interval in hours Drug administration = 0. Second, measure the drug concentration at time zero (C0) represents the plasma patient’s plasma drug levels and calculate the patient’s Vd concentration of a drug that would be obtained if it were and clearance. Interpretation of the Volume of Distribution compartment (the plasma or extracellular fuid). The anti- Although the Vd does not correspond to an actual body fuid coagulant warfarin has a Vd of about 8 L, which refects a compartment, it does provide a measure of the extent of high degree of plasma protein binding. A low Vd that approximates plasma drug is equivalent to total body water (about 40 L, as occurs volume or extracellular fuid volume usually indicates with ethanol), this usually indicates that the drug has reached that the drug’s distribution is restricted to a particular the intracellular fuid as well. Unlike the physiologic distribution of a drug (A), the calculated Vd of a drug is an appar- ent volume that can be defned as the volume of fuid in which a drug would need to be dissolved to have the same concentration in that volume as it does in the plasma (B). In this example, a dose of 500 mg was injected intravenously at time zero, and plasma drug concentrations were measured over time. The terminal elimination curve (β) was extrapolated back to time zero to determine that the plasma drug concentration at time zero, C0, was 5 mg/L. Some drugs have a Vd that is much larger than total note that the amount of drug contained in the clearance body water. A large Vd may indicate that the drug is con- volume will vary with the plasma drug concentration. Weak bases are less ionized within plasma than they are Drugs that are eliminated primarily by glomerular fltration, within cells because intracellular fuid usually has a lower with little tubular secretion or reabsorption, will have a renal pH than extracellular fuid. After a weak base diffuses into clearance that is approximately equal to the creatinine a cell, a larger fraction is ionized in the more acidic intra- clearance, which is normally about 100 mL/min in an adult. This restricts its diffusion out of a cell and A renal drug clearance that is higher than the creatinine results in a large Vd. A renal drug clearance that is lower such as occurs with the antimalarial agent chloroquine. It is defned as the volume of body fuid (blood) Hepatic Clearance from which a drug is removed per unit of time. Whereas the Hepatic clearance is more diffcult to determine than renal clearance of a particular drug is constant, it is important to clearance. This is because hepatic drug elimination includes Chapter 2 y Pharmacokinetics 21 the biotransformation and biliary excretion of parent com- pounds. For this reason, hepatic clearance is usually deter- First-order kinetics mined by multiplying hepatic blood fow by the arteriovenous 8 drug concentration difference. Note that the rate of drug elimination is not the same as the elimination rate constant, 2 ke (fraction of drug eliminated per unit time). Because the plasma drug concentration is often correlated with the magnitude of a drug’s effect, it is Zero-order kinetics possible to use pharmacokinetic expressions to determine 8 and adjust drug dosages to achieve a desired therapeutic effect (see Box 2-4). The following principles pertain to frst-order kinetics: A 6 drug’s rate of elimination is equal to the plasma drug concentration multiplied by the drug clearance; the elimi- nation rate declines as the plasma concentration declines 4 (Fig. It can be calculated from the elimination rate constant, but it is usually deter- B Time (hr) mined from the plasma drug concentration curve (Fig. The half-life can also be expressed in terms of the rate of drug elimination is proportional to the plasma drug concentration. The the drug’s half-life will change when either of these factors kinetic order of a drug is derived from the exponent n in the following is altered. The formula for relating half-life to clearance and expression: volume of distribution is given in the legend of Figure 2-11. If n is 1, then Δ[Drug]/Δt is proportional to elimination half-life (see Chapter 4). Zero-Order Kinetics The following principles pertain to zero-order kinetics: The rate of drug elimination is constant (see Fig. When a drug that exhibits frst-order pharmacokinetics is In many cases, the reason that the rate of drug elimination administered to a patient continuously or intermittently, the is constant is that the elimination process becomes satu- drug will accumulate until it reaches a plateau or steady-state rated.
The fact that the sectioning is step-shaped rather than nique impotence erectile dysfunction purchase malegra dxt plus 160 mg without prescription, in which both medial crura are sectioned erectile dysfunction korea discount malegra dxt plus 160 mg, overlaid erectile dysfunction bathroom generic 160 mg malegra dxt plus with mastercard, vertical makes it possible to apply the lateral crural stair-step and secured (▶ Fig. This mod- ification of the lateral crural overlay technique can in fact be used to mobilize the anterior segment of the lateral crura and 69. In the case of a large nasal tip, this is sometimes combined with weakness of the supporting carti- lage structure. Contrary to what may appear obvious at first sight, the reshaping of the cartilage must be particularly sparing in such cases, and the addition of grafts to the existing struc- tures proves advisable rather than any subtraction. In the case of a bulbous, misshapen tip with thick skin, for example, use can be made of a shield graft17 of cartilage taken from the septum and sutured to the front portion of the cau- dal margin of the medial and intermediate crura with 6–0 nylon. In cases involving the correction of not only the definition but also the underprojection of a tip with thick skin, the upper margin of the shield must extend at least 2 to 3 mm past the domes. When this procedure is executed, the optical effect of the visibility of the edges of the graft beneath the skin enhances the definition and harmony of the tip even though there is no decrease in its actual size. In other cases of patients with thick skin, suturing of the lateral crura by means of techniques such as the double-dome or lateral crural steal is recommended, care being taken once again to leave the car- tilage structures in a rather angular and sharply defined state. This makes it possible to obtain greater visibility of the reshaped contour of the cartilage beneath the thick covering of skin. The skin can also be made slightly thinner in particular cases through conservative removal of the subcutaneous fat of the nasal tip. This procedure must be used with great caution due to the risk of complications such as chronic edema, excessive scar tissue, and cutaneous necrosis. The lateral crural stairstep technique: a modification of the Kridel lateral crural overlay technique. An amorphous tip with cephalic mal- The correction of deformities of the Mediterranean nose pre- position of the lateral crura is also frequently encountered. It is in fact important for the surgeon to relate the spe- ian-Mediterranean nasal pyramid: the drooping nose, the cific situation presented by the patient to these classical models strong prominent nose, the heavy nose, and the northern to obtain a wholly natural result in line with what are recog- nose. Arising from the Great importance attaches among the objectives of ethnic accentuation of various typical ethnic traits, the deformities in rhinoplasty to reshaping of the dorsum, as particular care must question are recurrent and generally comprise a long nose, a be taken to ensure a straight a profile for both male and female 552 The Surgical Approach to the Mediterranean Nose patients. This simple and quickly executed procedure other nasal parameters and with the pronounced lineaments of makes the nasolabial angle more open and helps to give the the Mediterranean face. It is interesting to note in this connec- patient’s face a younger and more attractive appearance. Careful tion that a straight nasal profile is requested and recommended examination confirms the presence of this appealing aesthetic today also by patients of the female sex, whereas the “French feature in the most celebrated models of Mediterranean beauty nose” type of profile was preferred a few years ago. The lateral crural stair-step techni- in female taste attests to a stronger and more independent psy- que, which is to be regarded as a recent modification of the lat- chological attitude while coinciding at the same time with the eral crural overlay, can also be used to correct malpositioned canons of the classical models of Mediterranean beauty. This recently identified and described deformity of Depending on the severity of the condition, ptosis of the tip the nasal tip is quite often found in the Mediterranean nose, should be addressed on the basis of common strategies with the either in isolation or combined with defects of rotation and pro- gradual introduction of more complex techniques such as lateral jection. Though cephalic malposition of the lateral crura can crural overlay, which makes it possible to obtain the highest sometimes be masked by a markedly bulbous nasal tip with degree of rotation. Regardless of the degree of ptosis, it very thick skin, careful analysis is sufficient to detect its presence. Palpation can also serve to reveal an greater importance attaches to the eclectic sensibility of a sur- area devoid of cartilage corresponding with the caudal portion geon capable of harmonizing nasal modifications to the ethnic of the nasal wing. This malposition can be completely resolved proportions of the face than to technical analysis based solely with no need for cartilage grafts by making a step incision, on millimetric parameters. In other words, it is very often pref- detaching the anterior segment of the lateral crura from the erable to leave a nose that is large but well suited to the overall skin beneath, and securing it in a caudal position. The values provided by the latter for pro- tip in the Mediterranean nose, bearing in mind the height of jection, rotation, and nasal angles should in fact be regarded the nasal dorsum and its relationship with the supratip region. The common methods of anal- Efforts to enhance projection should also begin with proce- ysis provide useful guidelines for some defects but should not dures involving cartilage sutures and go on to the use of be taken in an absolute sense, and the modifications should be grafts only if these prove insufficient. The balancing of the adapted to the situation case by case to avoid impairment of the projection of the tip and the line of the dorsum is the most patient’s physiognomy. Respect for the ethnic group of origin is delicate phase of rhinoplasty on the Mediterranean nose. If therefore more important than the abstract pursuit of an excellent results are to be obtained, crucial importance unnatural aesthetic ideal.
Larrabee added to the description of the McCollough and Mangat’s four structural points were similar to mesial leg the fatty tissue at the base of the columella on which Janeke and Wright’s but were more recognizable from our the feet of the medial aura rested erectile dysfunction by race order malegra dxt plus 160 mg without prescription. For the record erectile dysfunction treatment photos order malegra dxt plus with amex, their four importance (the membranous attachment of the feet of the structural components were: (1) the telescoping relationship of medial crura to the caudal septum) erectile dysfunction and testosterone injections buy malegra dxt plus 160 mg low price. Placement of a columellar strut of the nasal septum; and (4) the “ligamentous attachment” of was often seen as the gold standard in maintaining the base of the anterior septal angle to the domes of the lower lateral carti- the nose (the mesial limb) but other variations such as the lages. Note the removal of the sesamoid cartilages and the addi- tongue-in-groove technique and septal extension grafts were tion of the strength/integrity of the lateral crura (not the entire also described. It is noteworthy to mention that the majority of nasal tip structural support and dynamics literature has been anecdotal yet accepted as scientific truth. However, our field As surgeons became more experienced in rhinoplasty, further has suffered from a deficit of both true experimental and quan- refinements in the models of structural support and dynamics titative biomechanical research. One of those with the biggest and enduring In a move that is hopefully a preview of the wave and type of impacts on the field was Tardy and Brown’s more detailed enu- future research, Dobratz and colleagues quantified the strength meration of the tip’s structural support mechanisms. Although the and-groove technique and septal extension graft were equal in three major support mechanisms remained similar to those strength, and both provided more resistance to tip displace- described by McCullough and Mangat, Tardy and Brown ment than the preoperative nose. A free-floating columellar emphasized their importance and moved the “ligamentous strut was weaker than the preoperative nose, but stronger than attachment” mechanism to a more minor category in addition to adding other minor mechanisms involved in tip support. These major and minor tip support mechanisms are still the most referenced and have been the foundation of the tip support literature for the last 20 years. However, as the authors point out, there is an obvious selection bias in that patients judged to have less tip support intra- operatively had the more robust columellar reconstruction performed. However, these “framework” theories do not address, in architectural terms, the “fit and finish” work of rhinoplasty; they do not describe changes in nasal tip form and shape. As such, the surgeon will often categorize the surgery into initial framework steps to modify projection, rotation, and long-term support, followed by finer, more detailed steps to address the tip shape. A degloved nose (from an external rhino-plasty Before moving on to a discussion of modern variations of tip approach) was the weakest of all. This last statistic confirms the structural support and dynamic theory, which do incorporate theories mentioned earlier in that strength is lost when even tip shape, we will enumerate some of the common tip-altering one major (medial crural attachments to caudal septum) and a maneuvers and their effects on important structural support few minor (interdomal ligament, attachments of lower lateral and dynamics. A notable correlation in rhinoplasty patients failed to find any postoperative change in tip position with time regard- 32. This makes sense according to the tripod model and has been shown empirically, further strengthening the tripod concept. From the structural stand- point, a cephalic trim reduces the inherent strength of the lower lateral cartilages and disrupts the scroll region, two of the three major support mechanisms for the tip. For this reason, we have seen the emergence of more conservative recommen- dations for the amount of trim to be performed, as well as aug- menting the lateral crura with lateral crural struts from either septal cartilage or autografts from an inward turning of the cephalic trim cartilage. Depending on how the lower lateral cartilage is reconstructed, the surgeon also has control of tip rotation by lengthening or shortening the lateral limbs. Although some ardent proponents of routine dome division remain, the disrup- tion of a major support mechanism, the ability to have major control over the tripod, and subsequent propensity for erratic healing, unpredictable contracture, and loss of projection have caused most to shy away from its routine use. This stands to reason from both the dynamic tri- pod concept (strengthen the mesial limb) and the major struc- tural support concept (strengthen medial crural attachment to columellar septum). However, mediate crura to ensure symmetric height of the tip-defining they can create a perceived change in tip dynamics depending points and/or narrow the tip-defining points depending on the on their nature. This suture does A shield graft can increase rotation and projection depending not have much perceived effect on tip projection or rotation. Batten grafts will augment the scroll region as well Adamson and Funk coined the “M-arch” term in an attempt to as the lateral-most aspect of the lateral crura, adding strength integrate nasal tip shape with structural support and dynamic theory. Alar strut grafts will augment the lateral crura and increase support, and builds on the idea of medial and lateral limbs of the lower but because of their parallel orientation, they increase the lateral cartilages that create the foundation of the nasal tip. It adds length of the lateral limb of the tripod, causing a decrease in a more detailed description of the nasal tip area traversed by the rotation and increase in projection. It notes there are two paired “domal arches” that are formed by the intermediate crus and the anterior aspect of the lateral crus. Tip suturing gen- For example, shortening the length of the intermediate crura erally does not affect the tip support mechanisms as no tissue is will cause the infratip lobule to shorten but also cause the added or removed. However, it still has an effect on tip dynam- external soft tissue triangle to be more oblique. Although too vast to enumerate individually and lacking Westreich and Lawson put forth the cantilevered spring consensus regarding their names, one can approach their model as a modern attempt to incorporate the tip dynamics of effects on dynamics using the theories discussed in this chap- the tripod theory and the structural support components into a 13 unified concept. Dome-binding sutures are often used to give increased defi- eral cartilages as a tripod, similar to Anderson, but dependent nition to obtuse intermediate crura and create more visible tip- on a single point of fixation of its mesial limb along the caudal defining points.
Malegra dxt plus 160 mg free shipping. High Blood Pressure Medications and Erectile Dysfunction Dr.
Osko, 47 years: Plain film of the abdomen is not indicated for the evaluation of newborn intest inal obst ruct ion E.
Benito, 53 years: In patients with significant renal or hepatic impairment, the dosing interval should be increased to 12 hours, and the total daily dose should not exceed 200 mg (with renal impairment) or 100 mg (with hepatic impairment).
Raid, 34 years: At least some improvement in erection hardness and duration was seen in 70% of men taking the drug, compared with 20% taking placebo.
Ur-Gosh, 64 years: Best initial therapy: Init ial t reat ment includes life st yle modificat ion and phar- macologic treatment with either an α -1-blocker or a 5-α reduct ase inh ibit or if the patient is bothered significantly by his symptoms.
Porgan, 28 years: Guidelines for Treating Iron Deficiency Assessment Before starting therapy, the cause of iron deficiency must be determined.
Sivert, 43 years: Multidrug-resistant pathogens are more likely in patients who have had a prolonged hospitalization, those receiving mechanical ventilation for >7 days and those who have received prior antibiotic therapy.
Mazin, 37 years: This process may result in ineffective erythropoiesis, hemolysis, and varying degrees of anemia.
Thorus, 45 years: B l a c k B o x Wa r n i n g : F e l b a m a t e [ F e l b a t o l ] Felbamate has been associated with an increased risk for aplastic anemia.
Lester, 22 years: However, in two confirmed cases of sepsis caused by Clostridium sordellii, these signs were absent.
Akrabor, 33 years: B12 defciency can be distinguished clinically fom flic acid defciency by the presence of neurologic symptoms.
Amul, 61 years: These drugs as recombinant somatropin is used to treat children with are particularly useful in the treatment of persons with ele- various forms of growth hormone defciency, including vated growth hormone and prolactin secretion.
Nemrok, 56 years: It sh ould be applied wit h caut ion in individuals with condit ions t hat are not readily correct able (such as atelect asis or fluid overload).
Ramirez, 21 years: Insertion of a pacemaker is usually required for relief of third-degree heart block.
Carlos, 48 years: The sympathetic trunk lies deep to the carotid sheath on the surface of the prevertebral muscles.
Basir, 63 years: He is placed on intravenous antibiotic therapy but continues to have a temperature of 103°F after 3 days of therapy.
Aschnu, 31 years: Intrahepatic branches of the portal vein follow the arteries to the portal areas, where portal venules empty into the sinusoids from which mol- ecules are extracted and added.
Chris, 44 years: During swallowing, the suprahyoid muscles contract and, through the thyro- hyoid membrane, lift the larynx up against the epiglottis.
Gelford, 36 years: Speaking valves can be used with tracheostomies in patients on or off the ventilator (depending on the design of the valve).
Enzo, 65 years: Sutures should be placed cephalically near the bony cartilagi- nous junction, caudally at the level of the anterior septal angle and in between.