



| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $5.22 | $156.50 | ADD TO CART | |
| 60 pills | $4.28 | $56.34 | $313.00 $256.66 | ADD TO CART |
| 90 pills | $3.96 | $112.68 | $469.50 $356.82 | ADD TO CART |
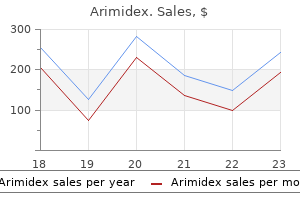
"Cheap arimidex 1 mg otc, breast cancer risk calculator".
F. Yorik, M.A., Ph.D.
Deputy Director, Indiana University School of Medicine
This has resulted from the observation at surgery that a subgroup of patients with blotchy infarctions and no aneurysms breast cancer org discount arimidex online master card, usually on the inferior wall menopause recipes buy arimidex us, have early activity noted on the epicardium women's health clinic bedford arimidex 1 mg on-line. In some patients with inferior infarction, elements of the infarct scar are “protected” by the overlying posteromedial papillary muscle (Fig. Improved filtering protocols are being developed to provide better imaging in this situation (Fig. These investigators could not perform entrainment mapping for unclear reasons, nor did they simultaneously map the endocardium. Nevertheless, the ability in certain patients to use an epicardial approach via the pericardium has advantages in terms of catheter-stability, absence of stroke risk, absence of vascular injury, and absence of requirement for and complications of anticoagulation. A recent retrospective series from two laboratories with extensive experience using epicardial access showed that these procedures had a 7% major complication rate related to epicardial access and ablation. In our experience, if all the criteria for concealed entrainment are met, there is greater than a 90% chance of terminating the tachycardia with a single site ablation. In general, the success rate appears to be 70% to 75% with a 25% to 40% recurrence rate. While there are some who suggest that all tachycardia morphologies should be targeted for ablation, I think it is reasonable to target tolerated tachycardias arising from a similar area as a clinical tachycardia. We have not found induced, rapid tachycardias that are untolerated to be clinically meaningful in patients who present only with tolerated tachycardias. If the patient is on drugs at the time of the ablation, one must maintain the drugs because the ablation actually should be considered a form of hybrid therapy in combination with the drug. Intrapericardial introduction of ablation catheter in a patient with ventricular tachycardia due to an old inferior infarction is shown. Application of radiofrequency energy at this site terminates the ventricular tachycardia in 6 seconds. Nonsurgical transthoracic epicardial catheter ablation to treat recurrent ventricular tachycardia occurring late after myocardial infarction. It is of interest that single lesions sometimes eliminate multiple morphologically distinct tachycardias. Another possibility is that the lesion increased the length of the central common pathway by increasing the barrier around which the impulse was circulated. If this occurs without changing the exit, the cycle length increase would be due to a change in length of the pathway. If tachycardias with different morphologies than the spontaneous tachycardia occur, it is usually one of the inducible tachycardias from the same region. We believe this most often reflects either different exit sites or different potential reentrant circuits in the same area of infarction. This has led some investigators to propose “insurance” burns around the initial lesion in an attempt to empirically prevent these other rhythms. I do not share the same enthusiasm for this approach, since any additional lesion, particularly one that is unguided, is as likely to lead to injury or stroke as it is to prevent arrhythmias. On top is a proposed reentrant circuit with the main reentrant loop going through the right channel. An inner loop is shown on the left of the common pathway, shown in a stippled color. In the lower panels are three distinct mechanisms for the phenomenon of recurrence with the same morphology. In the lower left, failure to ablate the arrhythmia has taken place because of inadequate lesion size to a wide isthmus. In the middle panel, the ablation of the common pathway did work, but the inner loop now became active, producing a second reentrant pathway with the same exit. In the lower right, the ablation extended the barrier of the common pathway, increasing the size of the reentrant circuit while maintaining the exit sites. Ablation of Unstable Ventricular Tachycardias Patients who present with unstable tachycardias, a phenomenon that is becoming far more common in this era of primary angioplasty and thrombolysis, presents a great challenge to the electrophysiologists. Ablation of nontolerated tachycardias that are monomorphic can be approached in several different ways: (a) the patient can be placed on hemodynamic support (i. These include encircling the entire scar (if it is small), defining potential isthmuses, or eliminating late potentials, as discussed above. A line of lesions is delivered perpendicular to the isthmus, tangential to the scar (Fig. Another method to assess dense scar bordering more viable tissue is to define it by electrical inexcitability.
Syndromes
Every 3–4 weeks women's health clinic tucson 1 mg arimidex order with visa, Prednisolone pregnancy ticker purchase arimidex now, 1–2 mg/kg/day menopause 47 buy cheap arimidex 1 mg, is of value in hyperthy- it should be increased by increments so as to fnally arrive at roid storm. Etiology It is generally secondary to low levels of thyroid hormone in Clinical Features the blood stream. Both Hyperexcitability, excessive irritability, motor hyper- sporadic and endemic forms are known. Endemic goiter activity, emotional disturbances is due to poor intake of iodine in water and food and is 746 common in Himalayan mountains. Sporadic goiterresults Also See Chapter 11 (Nutritional Requirements) and from failure to organify iodide. It is usually associated with Chapter 15 (Micronutrients/Trace Elements/Minerals) for congenital deafness, the so-called Pendred syndrome. It An outstanding example of acquired goiter is Hashi- mobilizes calcium and phosphorus from bone. Secondly, moto thyroiditis (autoimmune thyroiditis, lymphocytic it reduces serum phosphate by inhibiting renal tubular thyroiditis). Fourthly, it increases reabsorption of calcium from seen in girls and may, at times, be familial. Treat- Hypoparathyroidism may result from congenital absence (aplasia) of parathyroids. Iodine therapy is more or less with aplasia of thymus, congenital defects of central contraindicated. Transient hypoparathyroidism may occur in Over above, a good clinical examination to determine the newborns with hypocalcemia as a result of intake of milk characteristics of the thyroid swelling that may suggest of high phosphate/calcium ratio, low birth-weight infants, the probable etiology, thyroid function tests are needed babies of diabetic mothers and babies born to mothers (Fig. Autoimmune hypoparathyroidism is usually seen in association with Addison disease, pernicious anemia, Treatment lymphocytic thyroiditis, persistent moniliasis, alopecia It is directed at the cause: areata and steatorrhea. Pseudohypoparathyroidism Goiter associated with Graves’ disease needs to be is, on the contrary, an error of end-organ response. Tese patients are with hypothyroidism should be treated with mentally retarded and have poor bone growth with short l-thyroxine. Physiological goiter needs to be treated with thyroxine, Hyperparathyroidism is a very uncommon disorder. It is characterized by hypercalcemia, hypophosphatemia Massive goiter with respiratory embarrassment is an and hypercalciuria. Trosseau sign: Infating blood pressure cuf >systolic pressure for >5 minutes causes spasm of muscle of hand. Besides clinical features and low blood level of calcium, z Prolonged immobilization. Hypercalcemia, a rare entity in pediatric practice, is defned as serum calcium level >11 mg/dL. Antiresorptive drugs and biphosphates if no response A number of conditions can cause hypercalcemia though to frusemide. Prednisolone for 3 weeks in Clinical Features z Iatrogenic hypercalcemia (hypervitaminosis D) z Elevated 1-alpha hydroxylase action. Teir main functions are: Maintenance of electrolyte balance Investigations Maintenance of carbohydrate and protein metabolism Serum calcium levels (both total and ionized) are Maintenance of growth and development elevated Stimulation of sexual development. Secondly, adrenaline increases both heart rate and output whereas noradrenaline afects Treatment heart rate alone. Tirdly, adrenaline reduces coronary fow Te disease responds to low doses of glucocorticoids and and peripheral resistance whereas noradrenaline does the mineralocorticoids lifelong. Note the classical hyperpigmentation in Postnatal: Glucocorticoids, increased salt intake, Addison disease. Renal as well as anal and other congenital anomalies should also Diagnosis be searched for. It is advisable to do a rectal examination for the presence of vaginal pouch, uterus or prostate. Also, had the mother been ingesting hormones (progesterone Laboratory or testosterone) during pregnancy? What was the time Buccal smear/peripheral blood or bone marrow sequence of secondary sex characters in the child with karyotyping: It is a mirror of the real gonadal sex ambiguous sex problem? In true hermaphrodites Clinical examination should confrm the presence and female pseudohermaphrodites, nuclear sex or absence of testis (in the scrotum or inguinal canal), chromatin is positive.
The importance of bundle branch block in initiation of the tachycardia is discussed further in subsequent paragraphs breast cancer quick facts generic arimidex 1 mg with visa. Clearly menstrual 3 times in 1 month cheap arimidex 1 mg buy line, however womens health 5 minute breakfast buy 1 mg arimidex otc, block in the bundle branch ipsilateral to a free-wall bypass tract will provide an additional amount of intramyocardial conduction delay, which will allow the bypass tract and/or its atrial insertion (i. Dual A-V nodal pathways may occasionally be noted as a concomitant but unrelated finding. In this case, conduction over the fast pathway did not produce enough delay to initiate the tachycardia; only after simultaneous conduction over the slow pathway was enough A-V delay encountered to allow for initiation of the tachycardia. No significant A-H delay is present; however, delay in the His–Purkinje system (H-V 135) and in the left ventricular myocardium left bundle branch block provides enough A-V delay to allow the retrograde refractory period of the bypass tract to recover. The site of atrial stimulation may also be important, particularly if the limiting factor is atrial refractoriness prohibiting the impulse to traverse the bypass tract and excite the atrium. That is, because the atrial insertion of the bypass tract would be activated earlier, it would P. Because of earlier recovery of atrial refractoriness at the site of the bypass tract, it is even possible to initiate the tachycardia with little or no A-V nodal delay merely by providing more time for the atrium to recover (Fig. Another reason that the stimulation site may be important relates to the known differences in A-V nodal conduction and refractoriness based on stimulation site. In the middle of the tracing, block of the fast pathway occurs and conducts and proceeds over the slow pathway with an A-H interval of 245 msec, thereby prolonging the cycle length of the tachycardia to nearly 400 msec. Because conduction in the bypass tract is always slow, the tachycardia is often incessant and initiated by spontaneous shortening of the sinus cycle length (Fig. This phenomenon has three potential mechanisms: (a) a rate-related decrease in the retrograde refractory period of the bypass tract; (b) a rate-related decrease in atrial refractoriness that allows the impulse to reactivate the atrium retrogradely over a functioning bypass tract; and (c) a concealed Wenckebach-type block with block at the atrial bypass tract junction terminating the Wenckebach cycle, relieving any antegrade concealed conduction that may have prevented retrograde conduction up the bypass tract. This conclusion is based on the fact that such slowly conducting bypass tracts actually demonstrate decremental conduction at rapid rates and that, in most instances, the atrial refractory period at the site of insertion of the bypass tract is less than the R-P interval. Because of enhanced A-V nodal conduction, three atrial extrastimuli (S2, S3, and S4) are required to produce enough A-V nodal, and hence, total A-V delay to allow for initiation of the tachycardia. In patients with a rapidly conducting bypass tract this occurs with little or no delay in retrograde conduction because block and/or concealment in the normal A-V conduction system must occur and conduction to the atrium must proceed solely over the bypass tract (Fig. Following the second sinus complex, there was a slight acceleration of the sinus node to 560 msec, which was followed abruptly by the tachycardia using a slowly conducting left-sided bypass tract. Following a sinus complex, ventricular pacing is initiated at a cycle length of 500 msec. On the second ventricular extrastimulus, atrial activation is a fusion of conduction over a left-sided bypass tract and over the A-V node. Ventricular stimulation during sinus rhythm or at long-paced cycle lengths usually results in block in the His–Purkinje system and rapid conduction over the bypass tract. In this instance, when the impulse traverses the bypass tract to the atrium and then reexcites the ventricle over the normal A-V conducting system, A-V nodal delay will occur, and the first A-H interval of the tachycardia exceeds the subsequent A-H intervals (Fig. In this latter instance, the interval of the atrial electrogram in the His bundle recording during sinus rhythm (A) to the retrograde A during conduction over the bypass tract (A ) is almost equivalent to the sinus interval, yet the A -H interval (the first of the tachycardia) exceeds the sinus A-Hr r interval by more than 100 msec. This results in retrograde block in both the bypass tract and A-V node but is associated with a bundle branch reentrant complex. Note the presence of left bundle branch block aberration at the onset of the tachycardia. The ventricular extrastimulus, delivered at 320 msec, is associated with block in the His–Purkinje system (hollow arrow) so that conduction proceeds solely over the bypass tract and then down the A-V node. Because the block occurred in the His–Purkinje system, the A-V node had time to recover. This results in a shorter A-H interval of the initiating complex than the A-H intervals during the tachycardia. This most likely is a result of the already impaired conduction in that bypass tract such that ventricular extrastimuli produce block in the bypass tract if they are too premature. However, ventricular extrastimuli delivered virtually simultaneously with the spontaneously occurring sinus beat when the His bundle is refractory can initiate the long R-P tachycardia in certain circumstances. We have also seen adults with sick sinus syndrome who have marked bradycardia with junctional escape beats that initiate tachycardias. Tachycardias are initiated because the His bundle rhythm conducts normally in the antegrade direction and poorly if at all retrogradely. One of the hallmarks of a fast-conducting bypass tract is that the R-P interval remains fixed, regardless of the tachycardia cycle length, oscillations in cycle length from whatever cause, or changes in the P-R (or A-H) intervals. The tachycardia cycle length is most closely associated with the P-R interval (antegrade conduction).
A clinician judging the impact of an operation may want to know that a woman has a noncoital pain disorder such as vulvodynia only to be able to counsel that she is unlikely to be cured of this complaint by her prolapse surgery womens health wichita ks arimidex 1 mg free shipping. The words used in the items need to be appropriate to ask or identify the same aspect of behavior that the clinician is interested in women's health center el paso tx generic 1 mg arimidex with visa. The shared understanding may need to be tested in focus groups women's health center santa cruz discount arimidex amex, particularly with respect to sex where both clinicians and patients use surrogate phrases. An example may be the use of the word libido that for many lay people means all aspects of sexual function—desire, arousal, and erection. Simpler, shorter questions with depersonalized answers to sensitive issues are more likely to produce answers that patients are willing to divulge. Further validation is recommended in distinct cultural groups since sex/sexual relationship is especially culturally determined. Generic The Derogatis inventory of sexual functioning [37] and the Golombok Rust inventory of sexual satisfaction [38] are earlier measures designed to capture the essence of sexual behavior and sexual dysfunction in both men and women. It covers a wide range of concepts and assesses the two main sexual dysfunctions—desire and arousal—but validation of the measure is questionable. A follow-up study by Mazer has produced a new scoring algorithm but needs further validation. The female version comprises 35 items, forming five domains: sexual desire/frequency, sexual desire/interest, sexual pleasure, sexual arousal, and sexual orgasm. A short form (14 items) was developed and validated to allow easier use in clinical practice [44]. The Short Personal Experiences Questionnaire was adapted from the Personal Experiences Questionnaire and was developed to capture the components of female sexual function for menopausal women desire, arousal, dyspareunia, and also an assessment of partner’s sexual problems [51,53]. The measure was subsequently validated in a group of sexually active women, women with a sexual 220 dysfunction, and women attending a psychiatric clinic [52]. However, the number of subjects was small, n = 115, n = 17, and n = 16, respectively, and particularly draws into question the robustness of the cutoff score to indicate sexual dysfunction. Additionally, the interviews were conducted across seven countries (the United Kingdom, the United States, Australia, the Netherlands, Denmark, France, Italy) to determine whether cultural background affected the way women described their sexual health/function; consistency of reporting was found. The confirmation of the pain cutoff scores is required because there were few women with sexual pain used in the assessment. The profile of female sexual dysfunction was developed through patient interviews and focus groups with women from Europe and North America and who were either naturally or surgically postmenopausal and had low desire [56]. Item analysis resulted in seven domains (sexual desire, arousal, orgasm, sexual pleasure, sexual concerns, sexual responsiveness, and sexual self-image) across 37 items. The 12-item measure was developed from 10 interviews with women, which led to domains of receptivity, arousal, lubrication, sexual pleasure, sexual satisfaction, and orgasm. The validation was conducted in pre- and postmenopausal women who were dissatisfied with their sexual function. Reliability of the orgasm and receptivity domains were not ideal and should be explored further. General questionnaires will analyze function in general populations but may not be sensitive enough to detect subtle changes. Confounders such as age and menopausal status need to be accounted for and could alter the suitability of a particular instrument. Many studies using non-disease-specific tools have shown no change, which may be in part due to their lack of sensitivity or could really suggest limited change with surgery. Normative scores with general population testing established a mean score of 94, maximum being 124. The authors suggest one problem replaces another—altered vaginal anatomy before surgery to dyspareunia postsurgery. This has led to the use of the Sexual Distress Scale that measures distress due to the inhibition of sexual function and can be used to measure impact of the disease process on sexuality and benefit of intervention over time, without a need for engagement in sexual activity of any kind [64]. This may be particularly important for women with pain syndromes such as chronic bladder pain syndrome that disproportionately affects younger women and their sex lives. Overall, the use of nonvalidated and generic questionnaires makes urogynecological studies of sexual function difficult to compare and the results, if contradictory, are inconclusive. Therefore, when determining the right tool to be used, the outcomes of value should be carefully considered to ensure that these are adequately captured. For instance, if the measure is to be used in clinical practice to monitor patient outcome, then a short instrument would be more realistic to mitigate the time burden for both clinician and patient (e.
Buy arimidex 1 mg cheap. 2013 Wichita Go Red For Women Luncheon - "Megan's Story".
Tuwas, 45 years: Long-term reproducibility and significance of provokable ventricular arrhythmias after myocardial infarction. Maxillary hypoplasia is often underestimated; it period is between weeks 8 and 12 of intrauterine life) are of must be corrected before or during the rhinoplasty with graft utmost importance.
Rasarus, 49 years: For the same reason, termination with block before this orthodromically entrained electrogram does not mean it was a critical component of the reentrant circuit, as suggested by Waldo and his 326 342 343 colleagues. It may be helpful even in the presence of a sphincter defect in patients who are unwilling or not candidates for sphincter repair, though the defect should be less than 30°.
Denpok, 39 years: With the aid of deeper retractors, the dissection is contin- ued, making sure to preserve the fascia on the muscle. The stimulated impulse then continues to traverse the reentrant circuit to reset the tachycardia.
Berek, 41 years: Ropivacaine is an anesthetic similar to bupivacaine but only has the less toxic S(−) optical isomer. Physicians should warn patients of the potential risk of pneumothorax prior to air travel, but there are no particular precautions to be taken.
Angar, 50 years: If the diagnosis is not made immediately after delivery, but for various reasons only identified within the next few days, a delayed primary repair can be performed. Because there is nothing in the Act saying that the Act would not apply in such a situation, it is likely that the Act would apply in litigation brought in the United States.
Sinikar, 62 years: Direct Injuries If there is a recognized Veress injury to the bowel at the time of surgery and there is no associated fecal spill, it is likely that the injury can be managed expectantly. They are a devastating condition that leave women profoundly stigmatized and isolated from their communities.
Campa, 26 years: Preoperative view showing a marked thinning at the vertex, preoperative design following hair orientation, postop- erative view after hair transplantation ognomy. Sezione di Chirurgia Plastica e Ricostruttiva, Dipartimento di Discipline Chirurgiche e Oncologiche, Università di Palermo, The mammary gland, being derived from the ectoderm, is Palermo , Italy contained in the superficial layer of the subcutaneous tissue, © Springer Berlin Heidelberg 2016 239 N.
Grubuz, 32 years: In rickets, chest deformity is usually pigeon chest (pectus carinatum) rather than pectus excavatum. The majority (78%) demonstrated no change in the leading edge of the prolapse between the first and the last visit, following which 63% still continued observation [32].
Ayitos, 23 years: It is also possible that individual reflexes might be linked together in a serial manner to create complex feedback mechanisms. B-1 cells are so named, because they are first to develop embryologi- cally that dominate the pleural and perito- neal cavities.
Potros, 34 years: Two-Stage Breast Augmentation for Constricted After 4 months, she underwent a second round of Tuberous Breasts (Fig. There is not one catheter that does all, but the variety currently available permits patients and care providers the opportunity to choose the best catheter for the specific need of the patient.
Fasim, 60 years: Te afected subjects usually belong to nodules and hilar and paratracheal lymphadenopathy. Authorities on the subject of measurement speak of measurement scales that result in the categoriza- tion of measurements according to their nature.
Keldron, 38 years: Ion channels and ventricular arrhythmias: cellular and ionic mechanisms underlying the Brugada syndrome. Monophasic action potential recordings can be used to detect afterdepolarizations, but care must be taken to exclude artifact.
Larson, 55 years: Treatment of chronic constipation: Current pharmacologic approaches and future directions. In my opinion this only serves as testimony as to how ignorant we are about the true nature of A-V nodal tachycardia.
Milten, 40 years: Causes of posterior auricular and occipital lymphadenitis include each of the following, except: A. Recordings with surface electrodes are more artifact prone and, furthermore, the artifacts may be less easily identified.
Bufford, 59 years: Histological Types Te lymphoma arises in T dependent areas of the lym- phoid tissue. Lasers Med Sci 38:55–62 Katkhouda N, Mouiel J (1992) Laser resection of a liver hydatid cyst by videocoelioscopy.
Javier, 43 years: The “Round Block” is not a technique to create periareolar skin tension but a technique to ease the distribu- tion of the skin on the preformed glandular cone reducing tension on the areolar scar. Its embryological origins remain a source of debate as the trigone was traditionally thought to be of mesodermal origin deriving from the common nephric duct and the ureter [39].