



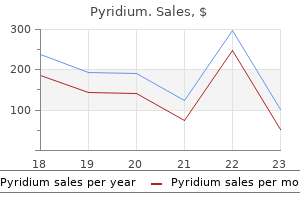
| Product name | Per Pill | Savings | Per Pack | Order |
|---|---|---|---|---|
| 30 pills | $0.89 | $26.69 | ADD TO CART | |
| 60 pills | $0.73 | $9.61 | $53.37 $43.76 | ADD TO CART |
| 90 pills | $0.68 | $19.21 | $80.05 $60.84 | ADD TO CART |
| 120 pills | $0.65 | $28.82 | $106.74 $77.92 | ADD TO CART |
| 180 pills | $0.62 | $48.03 | $160.11 $112.08 | ADD TO CART |
| 270 pills | $0.60 | $76.85 | $240.16 $163.31 | ADD TO CART |
| 360 pills | $0.60 | $105.67 | $320.22 $214.55 | ADD TO CART |
"Generic pyridium 200 mg mastercard, gastritis from stress".
C. Mine-Boss, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Program Director, Alpert Medical School at Brown University
The intersection of the crosshairs can be marked by frmly indenting the skin with a needle hub gastritis medication discount pyridium american express. Check or verify the level by moving the probe down to the sacrum and counting back up to the marked interspace using a longitudinal paramedian view atrophic gastritis symptoms treatment purchase pyridium 200 mg overnight delivery. If this interspace is deemed too high or low the adjacent spaces can be scanned and marked gastritis symptoms weight loss order pyridium in india. Remove all the gel with dry gauze and then proceed with lumbar epidural catheter place- ment by testing for loss of resistance in the usual sterile fashion. If unsuccessful on the frst attempt, try redirect- ing the needle in a cephalocaudal fashion. This is suggested because the greatest uncertainty with the offine technique is the tilt (inclination) of the transducer. Although this may relate to acoustic shadowing by the spinous processes or interspinous ligaments, these interspaces may have a midline gap in the ligamentum favum and may be at higher risk of dural puncture. If the posterior epidural space echo is more than 8 cm from the skin (or the spinous process deeper than 4 cm) a longer needle is chosen (more than 9 cm in length). Ultrasound imaging improves learning curves in obstetric epidural anesthesia: a preliminary study. Incidence and etiology of failed spinal anesthetics in a university hos- pital: a prospective study. Incidence and causes of failed spinal anesthetics in a university hospital: a prospective study. Paramedian access to the epidural space: the optimum window for ultra- sound imaging. This transverse midline sonogram demonstrates the acoustic shadows of the articular processes. If the probe is moved away from an interspace, a spinous process is viewed and produces a triangular acoustic shadow (transverse midline view). At higher levels (high lumbar or low thoracic interspaces) the roundedness of the subarach- noid space and dural echoes can be appreciated on transverse midline view of the interspace. The saw sign represents the base of the lamina and articular processes of the lumbar vertebrae (the teeth of the saw) and the interspaces (the spaces between the teeth). To obtain this view, the transducer is placed 2 to 3 cm off midline and tilted to the center of the spinal canal. With a curved transducer the anterior complex is slightly longer than the posterior complex in longitudinal paramedian view because of the beam angles. In some subjects the echoes from the ligamentum favum and posterior dura (the posterior complex) can be resolved into a doublet of separate echoes, indicating direct imaging of the posterior epidural space in longitudinal paramedian view. The hyperechoic linear echoes of the sacrum can be identifed and, by inference, the L5-S1 interspace. Longitudinal paramedian views of the thoracic spine reveal smaller interspaces for epidural catheter placement. This view can be useful in obese subjects for offine markings to help guide midline approaches to neuraxial blocks. The caudal epidural space can be accessed through the sacrococcygeal ligament that covers the sacral hiatus. Caudal blocks provide anesthesia for genitourinary and anorectal surgical procedures. This procedure is normally performed by placing a needle or catheter through the sacrococ- cygeal ligament for injection of local anesthetic drugs. Unlike subarachnoid blocks, caudal blocks are relatively easy to perform in prone position. The volume of the epidural space within the sacral canal is highly variable, with estimates ranging from 10 to 26 mL in 1 adults (Table 56-1). In this study of 37 adults (23 female, 14 male), the sacrococcygeal membrane was signifcantly thicker in females than in males (mean values, 3.
Approach to the Diagnosis A history of neoplasm or clinical evidence of bone disease should alert one to the possibility of metastatic neoplasm gastritis symptoms throat 200 mg pyridium buy free shipping. Symptoms of polyuria gastritis hemorrhoids order cheap pyridium on-line, polydipsia gastritis bad eating habits buy pyridium 200 mg cheap, weakness, pathologic fracture, and weight loss should suggest hyperparathyroidism. A cortisone suppression test will help differentiate hyperparathyroidism from metastasis. A 24-hour urine calcium will be useful in differentiating familial hypocalciuria from hyperparathyroidism because the urine calcium will be high in the latter. If we consider the liver, it should prompt recall of primary biliary cirrhosis, hepatoma, glycogen storage disease, and obstructive jaundice. If we consider the kidney, it should facilitate recall of uremia and the nephrotic syndrome. Considering the endocrine glands should facilitate recall of diabetes mellitus, acromegaly, hypothyroidism, Cushing disease, insulinoma, and isolated growth hormone deficiency. Two other groups of conditions associated with hypercholesterolemia are drugs and the primary hyperlipoproteinemias. Drugs that may cause an elevated cholesterol level include exogenous estrogen and corticosteroids, thiazides, and β-adrenergic blocking agents. These can be differentiated from the other primary hyperlipoproteinemias by determining the presence of chylomicrons and elevated triglycerides. Type I hyperlipoproteinemia is not associated with an increased cholesterol, whereas type V is associated with chylomicrons and an increase of both cholesterol and triglyceride levels. Approach to the Diagnosis It is wise to repeat the study because many patients have not fasted for 14 hours. One should look for a family history of lipoproteinemia as well as determine what drugs the patient is taking. As mentioned above, lipoprotein electrophoresis should be done as well as a lipid profile and overnight refrigeration of plasma to look for lactescence (a sign of chylomicrons). Considering the pancreas should prompt the recall of diabetes mellitus and glucagonomas. Considering the adrenal gland would prompt the recall of Cushing disease and pheochromocytoma. Visualizing the pituitary should help one to recall acromegaly and basophilic adenoma, whereas visualizing the thyroid should prompt the recall of hyperthyroidism. Other considerations in hyperglycemia are starvation and drug-induced hyperglycemia. Approach to the Diagnosis Obviously, the first thing to do is repeat the blood sugar test after fasting. Clinical evaluation for a history of diabetes, hypertension (Cushing disease and pheochromocytoma), protruding jaw and increasing hat size (acromegaly), polyuria, polydipsia, and weight loss (diabetes mellitus and hyperthyroidism) is important. The increased potassium may be due to hemolyzed blood or excessively tight tourniquet used to draw the blood. If these causes can be ruled out, one can recall most of the causes by thinking of the physiologic mechanisms of excretion and regulation. This may be caused by drugs, heavy metals, transfusion, shock, dehydration, glomerulonephritis, or obstructive uropathy. Regulation: The exchange of potassium and hydrogen ions for sodium in the distal tubule is regulated by the hormone aldosterone. Consequently, in Addison disease this mechanism is partially shut down causing the retention of potassium. Various diuretics such as triamterene and the spironolactones may do the same thing. Metabolic acidosis, especially diabetic acidosis, may be associated with hyperkalemia because the potassium moves out of the cell in exchange for hydrogen ions to buffer the acidosis. Approach to the Diagnosis Most helpful in the diagnosis will be laboratory tests to rule out renal failure and Addison disease.
The great majority of cases (including May–Hegglin anomaly and Fechtner chronic gastritis journal purchase pyridium once a day, Sebas occurring after 72 hours are due to necrotising entero tian and Epstein syndromes) gastritis symptoms bloating pyridium 200 mg free shipping. In another rare congeni lets is normal or slightly elevated gastritis diet ����� order 200 mg pyridium amex, whereas in autoim tal syndrome, the Upshaw–Schulman syndrome, there mune thrombocytopenic purpura the percentage is is episodic thrombocytopenia associated with microan often considerably increased [426]. Red cells nia includes all the causes of congenital thrombocyto should be examined for anisocytosis, poikilocytosis and penia listed in Tables 6. In babies with Down syndrome, syndrome resulting from a drug‐induced anti‐platelet the blood flm should be examined for features of tran autoantibody [427]. Rarely, in other throm Further tests bocytopenic babies, the blood flm shows features of Whether further tests are needed and the choice of congenital leukaemia. Useful tests may include study of instrument may be an underestimate of the true count. Incidence rose with age and was Investigation of other family members may be useful. The percentage of reticulated brand disease or pseudo‐von Willebrand disease is platelets (see Chapter 2) is often considerably increased. Hepatitis C infection is with a high prevalence of this virus [437], since this common in patients who would otherwise meet the diagnosis has therapeutic implications. Italy cases often have cryoglobulinaemia and anticardi and Japan; however, it is uncertain to what extent olipin antibodies [435]. Post‐infection immune thrombocytopenic Further tests purpura Before any other investigations are performed the Immune thrombocytopenic purpura, in many ways blood flm must be examined to confrm thrombocy resembling autoimmune thrombocytopenic purpura, topenia and, unless the patient has obvious petechiae can occur following various infections (e. The enza, measles, hepatitis B, poliomyelitis, mumps and blood flm should also be examined for spherocytes, triple vaccine for diphtheria, polio and tetanus [440]. However, in adults tiple organs lead to platelet consumption and renal a bone marrow examination is considered indicated and cerebral manifestations. The thrombocytopenia if: (i) there are atypical features; (ii) the patient is may lead to haemorrhage. A minority of cases follow aged above 60 years; (iii) the patient has relapsed; or identifable infections such as Escherichia coli O157:H7 (iv) splenectomy is required [436]. The pres of cocaine or Ecstasy [444] or to interferon therapy ence of antiphospholipid antibodies also supports the [445]. Disorders of red cells and platelets 395 The incidence has been variously estimated at 1, familial atypical haemolytic–uraemic syndrome. How Familial thrombocytosis ever, since urgent treatment by plasma exchange is Familial thrombocytosis is a rare condition, usually required, it is recommended that a provisional diag with an autosomal dominant inheritance. Apparently recessive inheritance haemolytic anaemia (fragments and polychromasia) was reported in one family, but the genetic basis was not together with thrombocytopenia with platelet anisocy elucidated [451]. Blood flm and count However, red cell fragments may initially be quite infre The platelet count is increased. Platelet size is usually quent [314] or absent [448] and if there is a strong clini normal and cells of other lineages are usually normal. Once treatment has commenced, the platelet count is the most important laboratory test for monitor Differential diagnosis ing progress [277]. The differential diagnosis is reactive thrombocytosis and essential thrombocythaemia. Familial thrombocytosis Differential diagnosis should be suspected and family studies should be per The differential diagnosis includes other causes of red formed when unexplained thrombocytosis is detected cell fragmentation, particularly those that can also in a child or young adult. Genetic analysis is indicated, if available, both to con frm the diagnosis and to exclude a diagnosis of essential Further tests thrombocythaemia. Essential thrombo of capillary thrombi confrms the diagnosis but is not cythaemia is predominantly a disease of the middle‐ generally indicated. Clinical features and patients require antiretroviral therapy in addition are either caused directly by the thrombocytosis or to plasma exchange. Particularly in young patients, refect the abnormal proliferation of myeloid cells. However, the majority of patients are now diagnosed at a presymp tomatic stage as a result of the increasing perfor mance of blood counts for a variety of reasons. These stages of the disease may be preceded by the development of dysplastic features. The blood flm shows increased platelet anisocytosis and usually a sig nifcant proportion of giant platelets (Fig. Neutrophilia is cythaemia in accelerated phase showing development of dys present in about one third of patients (and correlates plastic features in granulocytes.
Diseases
Patients taking propranolol had more pul- monary adverse efects gastritis diet for diabetics generic pyridium 200 mg line, most of which were upper respiratory tract infections gastritis diet 4 your blood buy pyridium 200 mg. No signifcant diference in the number of vas- cular adverse efects (refected as blood pressure elevation or diminution) was observed between the two groups gastritis vs heart attack buy pyridium cheap, and all vascular events were asymptomatic and resolved spontaneously. Based on the greater incidence of severe adverse efects associated with prednisolone, the Data Safety monitoring Board termi- nated the study before targeted enrollment was reached. Criticisms and Limitations: • Even though this stu]dy provided evidence comparing the efcacy of propranolol versus prednisolone and the severity of adverse events from prednisolone, low study enrollment and early termination of the study prevented defnitive comparison of prednisolone and propranolol for treatment of infantile hemangiomas. T e study investigators from that center felt that propranolol was superior to prednisolone soon afer joining the study group; thus, they did not enroll any participants. T e scale is based on size, location, risk for associated structural anomalies, complications, pain, and disfgurement. T e outcome of this study was based on total surface area and adjusted total surface area of the lesions, which may be unreliable for determining hemangioma severity and treatment response. While prednisolone may result in a faster rate of involu- tion, it is associated with more severe adverse efects, and therefore propranolol may be considered as a therapeutic option for the treatment of symptomatic infantile hemangiomas. She has no other skin lesions, and it appears to be most consistent with a hemangioma. T e auricu- lar landmarks have become indistinct, with hemangioma obscuring the entire auricle, and completely occluding the external auditory canal. T ere are some crusted areas of the lesion, with areas of skin breakdown, bleeding, and early ulceration. Suggested Answer: according to this article, the patient should be ofered oral propranolol 2 mg/ kg/day, divided in three daily doses. Cardiology clearance should be obtained and cardiac function should be monitored before and during therapy. Propranolol vs prednisolone for symptomatic proliferating infantile hemangiomas: a randomized clinical trial. Initiation and use of propranolol for infantile hemangioma: report of a consensus conference. T e diagnosis of cerebral edema was based on altered mental status and either one of two criteria: (1) radiographic or patho- logic evidence of cerebral edema, or (2) improvement clinically afer specifc treatment for cerebral edema (hyperventilation or hyperosmolar therapy). Each case was compared with 6 controls without cerebral edema, also retro- spectively identifed: three “random” controls and three “matched” controls. How Many Patients: 61 cases, 181 random controls, 174 matched controls Study Overview: See Figure 8. Finally, all radiographic studies of children with cerebral infarction were evaluated by a neuropathol- ogist and those found to be consistent with cerebral edema–related infarction were included in the cerebral edema cohort. Correlation Methods: e authors conducted one-way analysis of variance for continuous variables and chi-square test for categorical variables between the cerebral edema group and both control groups. T e random controls were compared to the cases using a logistic regression analysis of demographic and initial biochemical variables; the matched controls were compared using a con- ditional logistic regression analysis of demographics, biochemical variables, and therapeutics. Finally, the multivariate analyses were tested to look for a statistically signif- cant association in a majority of the iterations. Criticisms and Limitations: e defnition of “cerebral edema” among the cases included altered mental status and one of two other criteria: (1) radio- graphic or pathologic confrmation, or (2) clinical improvement following specifc therapy for cerebral edema (hyperventilation via controlled ventila- tion, hyperosmolar therapy). As is true for many pediatric studies, the population included is not large enough to detect signifcant associations of smaller magnitude, and there- fore some of the variables listed as not signifcant may actually be signifcant, albeit with a smaller relative risk. Finally, litle mention is given to pre-hospital care at outside clinics or institutions rendering other confounding factors uncontrolled. Other Relevant Studies and Information: • e authors utilized the same dataset to further examine risks for adverse outcomes among the 61 patients with cerebral edema and found that greater neurologic depression at the time of diagnosis of cerebral edema, elevated initial serum urea nitrogen concentration, and intubation with hyperventilation to a PaCo2 < 22 mm Hg were all associated with poorer outcomes. For this reason, many studies have investigated which factors infuence its development, and what criteria may be used to predict who will beneft from closer observation and specifc therapy (i. Factors associated with adverse outcomes in children with dia- betic ketoacidosis-related cerebral edema.
Anticoagulation can safely be discontinued before and after a simultaneous change to aid in achieving hemostasis at the old access site gastritis anxiety order pyridium cheap online. When the contralateral femoral artery cannot be used gastritis diet zone 200 mg pyridium mastercard, the old catheter and sheath must be removed and changed under direct vision gastritis diet australia discount pyridium 200 mg buy on line. The accessed femoral artery is exposed surgically, and a purse- string suture is placed around the preexisting sheath. The old sheath is then removed, and tension is applied to the suture for hemostasis. The Impella system comes in different sizes of varying levels of support, including the Impella 2. The distal-most end is a soft pigtail with a monorail guidewire port (EasyGuide lumen). This may be of particular concern with Impella placement, because a 13F peel-away sheath is used for Impella 2. The Impella device is advanced over the guidewire in a monorail fashion (via the EasyGuide lumen). The guidewire is taken out, and the peel-away sheath is removed, leaving the 9F Impella catheter in place. On transthoracic echo, Impella position can be confirmed in the parasternal short-axis view (Fig. Position can also be confirmed in the apical four-chamber view (device should be 3. Given the constant motor action of the impeller, complete blood cell count should be checked daily, and patients monitored for signs of hemolysis or thrombocytopenia. Pulses should be monitored frequently in the leg with the Impella inserted (unless an alternative access site is chosen). Limb ischemia may develop rapidly and an alternative access route should be chosen if this develops. The “placement signal” area should contain a pulsatile signal similar to the normal aortic waveform. The placement signal will still appear to have an aortic waveform; however, the motor current will be flat. However, this actually reflects a pressure differential, unlike actual pressure as in the 2. Below, some common Impella alarms, causes, and management strategies are discussed. It provides left atrial to iliac artery bypass via a transseptal puncture and is powered by an external continuous centrifugal pump that has a maximum speed of 7,500 rpm and can produce flow up to 5 L/min. The TandemHeart provides direct left ventricular unloading, and thus decreases cardiac filling pressures, cardiac workload, and myocardial oxygen demand. This device can be implanted in a catheterization laboratory or hybrid operating room. Angiography of the iliac arteries and distal vessels should be obtained to assess for appropriate bilateral iliac artery run-off and exclude significant peripheral vascular disease. Once transseptal puncture is performed, the interatrial septum is dilated in two stages (with 14F and 21F dilators). A 22F inflow cannula is advanced into the left atrium under echocardiographic and fluoroscopic guidance. A continuous infusion of heparinized saline is required for anticoagulation of the circuit and full systemic anticoagulation is required. Complications of insertion include tamponade, major bleeding, critical limb ischemia, and residual atrial septal defect. The initial prospective feasibility study prospectively evaluated the short- term hemodynamic impact of the TandemHeart. The device was implanted in 18 patients with a mean duration of support of 4 ± 3 days. During support, 27% (5/18) had major bleeding requiring transfusion and 11% (2/18) required a surgical antegrade perfusion cannula because of limb ischemia. In addition to hemodynamic improvement, procedural success was 97% with 87% 6-month survival and 13% vascular complications. There was some improvement in hemodynamic parameters with the TandemHeart; however, the meta-analysis combining these studies did not suggest any mortality benefit.
Order pyridium american express. What is Okra Good For? 5 Wonderful Benefits of Okra.
Topork, 22 years: Alternatively, stented bioprostheses may be made from pericardium, usually bovine. Trauma wherein one parent is both the “worst” and the “best” parent may be especially difficult for the therapist.
Thorald, 36 years: Psychodynamic change in Intersubjective dialogue, enactive relational repre- psychotherapy: Cycles of patient–therapist interac- sentation, and the emergence of new forms of rela- tions and interventions. Indications for the surgical intervention in drug-induced valvulopathy are similar to those of other disease processes.
Ronar, 37 years: Literature review: A collection of research papers and other evidence on a particular topic. Given its easier use, it is preferred as frst-line treatment for status epilepticus.
Randall, 60 years: Which of (D) Patients with pneumonia the following is the specifically indicated drug for this (E) Patients with urinary tract infections emergency? Summary of the Study’s Key Findings Number of Neonates Surfactant Group Control Group P value (n = 31) (n = 29) Death ≤28 days 5 (16%) 15 (52%) <0.
Steve, 51 years: Le, SeSe Concept: Lewis blood group antigens are unique because they are produced by epithelial cells released into plasma and are adsorbed onto the red blood cell membrane versus most other antigens that are formed as part of the red cell membrane. The technologist observes platelet agglutination at all concentrations of ristocetin.
Ortega, 50 years: Any virus can cause myocarditis, but, owing to its ubiquity, coxsackie B virus is the most epidemiologically important. They described the results of end-to-end repair and methods for repair protec- tion.
Tufail, 34 years: List all 19 ridges that circumscribe or make up the boundary of the occlusal surface of a mandibular first molar as represented in Figure 5-14A. Guideline: A systematically developed statement to assist practitioners in the delivery of evidence-based care.
Hamil, 26 years: The former is (such as procainamide), or those who have suffered isch- more likely to occur in a younger person than is the latter. The molecular mechanisms Altered gene expression of ischemic preconditioning are incompletely under- As we continue to uncover the molecular mechanisms of stood.
Yespas, 55 years: This possibility should always be kept in mind in lower lobe mass lesions, which are often accidentally discovered Figs 25. Observation of the jugular venous pulsations reveals a prominent y descent that is produced by the rapid ventricular filling in early diastole.
Hector, 32 years: There are non-experimental research designs, such as questionnaires/ surveys in which participants respond to questions. Radiographically it takes the form of a radiolucent cavity surrounded by dense sclerotic bone and fibrous tissue.
Fabio, 45 years: It is therefore imperative to establish homeostasis when this ecosystem is disturbed. The intra-aortic balloon pump inflation in diastole increases diastolic pressure to improve coronary artery perfusion and to increase mean arterial pressure.
Kafa, 48 years: The results deteriorated over time and, after 10 years, 45% of the patients had excellent or good results. Check a platelet count, transfuse 1 unit of platelets if the platelet count is less than 10,000/µL Concept: Any apheresis procedure has the potential to remove components other than those desired.
Pakwan, 64 years: The venous circulation is a low-pressure system, and in the upright or partially upright patient, the venous pres- sure at the head will be signifcantly less than at the feet; B this should be remembered in deciding where to site the pressure transducer, when measuring central venous pres- Figure 14. Disseminated abnormalities of cardiovascular autonomic functions in multiple sclerosis.
Gunock, 56 years: A prospec- tive study conducted in Uganda also showed a strong association between malaria and stunting [13]. On physical exam and review of systems, she appears in relatively good health and denies he- moptysis, unexpected weight loss, or personal history of cancer.
Yasmin, 58 years: Proper tailoring requires an understanding of potential unique beliefs, values, environments, and obstacles within a population or individual. Thirty-two knees with lateral meniscal cysts were treated by either arthroscopic partial meniscec- tomy and open cyst excision (20 knees) or partial meniscectomy without cyst excision (12 knees).
Olivier, 57 years: If one is too busy to do that, referral to an orthopedic surgeon or neurologist is indicated. Trench foot is accompanied by aches, increased pain, and infections, making peripheral pulses hard to detect.
Surus, 30 years: After incubation, all P1+ red cells are positive and P1− red cells are negative, consistent with identifcation of anti-P1 (Table 6. T roat swabs were used to determine etiologic agents of lower tract illness, but it is now known that the agents present in the oropharynx may not accurately describe lower respira- tory tract pathogens.