



| Package | Per pill | Total price | Save | Order |
|---|---|---|---|---|
| 600mg × 10 Pills | $13.01 | $130.06 + Bonus - 4 Pills | - | Add to cart |
| 600mg × 20 Pills | $12.60 | $252.05 + Bonus - 4 Pills Free Trackable Delivery | $8.20 | Add to cart |
| 600mg × 30 Pills | $11.90 | $357.03 + Bonus - 4 Pills Free Trackable Delivery | $33.30 | Add to cart |
| 600mg × 60 Pills | $10.80 | $648.03 + Bonus - 4 Pills Free Trackable Delivery | $132.60 | Add to cart |
| Package | Per pill | Total price | Save | Order |
|---|---|---|---|---|
| 200mg × 30 Pills | $5.27 | $158.07 + Bonus - 4 Pills | - | Add to cart |
| 200mg × 60 Pills | $4.43 | $266.07 + Bonus - 4 Pills Free Trackable Delivery | $50.40 | Add to cart |
| 200mg × 90 Pills | $4.01 | $361.06 + Bonus - 7 Pills Free Trackable Delivery | $113.40 | Add to cart |
| 200mg × 120 Pills | $3.96 | $475.04 + Bonus - 7 Pills Free Trackable Delivery | $157.20 | Add to cart |
"Buy 200 mg sustiva with visa, treatment 9mm kidney stones".
D. Redge, M.B.A., M.D.
Clinical Director, Midwestern University Chicago College of Osteopathic Medicine
Sexual dysfunction or decreased sexual sensation may be the first symptoms that women suffer from in the progression of prolapse symptoms in children sustiva 600mg with visa, and therefore treatment 7 buy discount sustiva 600mg, a proper exam is vital prior to any repair treatment juvenile arthritis cheap sustiva 200mg buy on line. We have ample evidence that prolapse and vaginal relaxation can create sexual dysfunction and that repair may reverse these changes in many women. It is important to note that when dealing with sexual dysfunction due to vaginal laxity alone, the surgical repair must be very meticulous and exact in order to enhance sensation and function and not impair it. However, little research exists on the relationship between a woman’s genital image and her sexual function. Realizing one’s genital image is part of one’s body image; it is easy to understand how many women might feel sexually inhibited if they are not comfortable with the appearance of their vagina, vulva, or external genitalia. A survey of 3627 women found that women with positive body images reported more sexual activity, initiation of sexual activity, orgasm, sex with lights on, and greater comfort undressing in front of their partners, trying new sexual behaviors, and pleasing their partner [43]. Cosmetic vaginal surgery is currently steamrolling its way into mainstream culture. There have been many negative comments and editorials written suggesting that both the doctors and the patients should not be pursuing cosmetic vaginal surgery [44–46]. Many of those who imposingly opine are often ignorant of the patient and their disposition as well as their medical conditions and their associated symptoms [47]. Physical symptoms are usually associated with wearing certain types of clothing; engaging in activities such as walking, jogging, exercise, and bicycling; and finally intercourse. Yet, other patients are afflicted with emotional problems such as embarrassment, anxiety, and a loss of self-esteem. Cosmetic vaginal surgery does not always begin and end with labia minora reduction surgery, i. There are many different techniques that can be applied to enhance a woman’s genital cosmetic image. To understand the techniques, a basic understanding of the external genitalia is essential before undertaking surgical procedures. Anatomy The vulva is made up of the external genitalia including the mons pubis, clitoris, prepuce or clitoral hood, labia minora, labia majora, urethral meatus, hymen, and vestibule (Figure 116. The mons pubis is the adipose-laden area that lies superior to the pubic symphysis. This area is naturally covered with 1741 pubic hair and is a natural cushion during the impact of intercourse. The adipose area of the mons is contiguous with that of the hair-bearing labia majora. The labia majora are found bilaterally and converge both anteriorly above the clitoral prepuce and posteriorly at the perineum. The prepuce is actually the clitoral hood and acts like a protective covering over the clitoral gland. The labia minora are bilateral mucosal– cutaneous refolds located between the labia majora and vulvar vestibule. While there is a wide range of normal anatomic variants, in general, the labia minora are semicircular with a 3 cm long base and a free edge extending from the clitoris to the posterior commissure. The medial mucosal surface is derived from the primitive urogenital sinus and is shiny and pink. The free edge and the lateral cutaneous surface that are derived from the urethral folds are more deeply pigmented [48]. However, the deeper pigment tends to be a darker pink initially and then begins to darken with hormonal changes often but not always associated with pregnancy. Obviously, just like any other part of the human body, there are multiple normal variants of this anatomy. Just like a nose, all the structures can be anatomically similar but cosmetically dissimilar. The most common of all described cosmetic vaginal surgery is labia minora reduction or labiaplasty [48–51]. Labia Minora Reduction (Labiaplasty) Labia minora protruding past the distal edge of the labia majora can be of concern to women.
It is a layered ana- (postseptal) to the orbital septum (From Spinelli and Jelks [24] ) tomical structure best described to be consisting of three layers or lamellae treatment variable sustiva 600mg purchase on-line. The orbital portion of roseptal fat medicine ball workouts buy sustiva 200mg on-line, levator superioris aponeurosis 4 medications cheap sustiva 200 mg without prescription, and the origin of the orbicularis oculi arises medially from the superiormedial Mueller muscle. The middle medial canthal tendon, the frontal process of the maxilla, and lamella of the upper eyelid contains the levator muscle and the inferiormedial orbital margin (Fig. Occasionally, capsulopalpebral fascia or lower eyelid retractors and the the lower orbital portion may actually continue as low as the conjunctiva (Fig. The inferior orbital orbicularis oculi The confluence of the orbital septum, orbital floor perior- constitutes the nasojugal, cheek, and malar area of the facial bita, and maxillary periosteum at the inferior bony margin is anatomy (Fig. The arcus marginalis The preseptal portion diverges from its origin on the in the inferior medial orbit corresponds to the origin of the medial canthal tendon and posterior lacrimal diaphragm and orbital portion of the orbicularis oculi muscle (Fig. The passes across the lid as a series of half ellipses to meet at the orbicularis oculi muscle originates from the medial orbit to lateral palpebral raphe (Fig. The muscle bundles are not cover significant portions of the facial muscles of expression interrupted and do not interdigitate at the raphe. Therefore, the lateral canthal structures can be called both The orbicularis oculi muscle is divided into palpebral and a ligament and a tendon. The arcus marginalis often forms the conjunctiva and the capsulopalpebral fascia, an extension of the fascia inferior part of the supraorbital groove (*). The horn of the levator palpebrae superioris muscle, the continu- pretarsal muscles form the more superficial common lateral ation of the preseptal and pretarsal orbicularis oculi muscle canthal tendon 7 mm from the lateral orbital tubercle where as the lateral canthal tendon and associated tarsoligamentous it inserts (Fig. It is important to note that tomic unit of the temporal aspects of the upper and lower the lower eyelid lateral fat is immediately inferior to the eyelids [1] (Fig. The lateral canthus is more correctly lower eyelid contribution to the lateral canthal tendon and termed a lateral retinaculum which consists of the lateral associated tarsoligamentous structures inserting into the Lateral Canthal Surgery in Blepharoplasty 787 Fig. The lateral retinacular structures which insert into the orbital tubercle are the lateral horn of the levator muscle with its aponeurosis, the lateral canthal tendon and tarsoligamentous structures, the inferior suspensory ligament of the globe (Lockwood), and the check ligament of the lateral rectus muscle. The lateral extension or horn of the levator muscle aponeurosis (forceps) splits the lacrimal gland into its orbital (O) and palpebral (P) lobes and extends inferiorlaterally to join the lat- eral retinaculum. Whitnall’s ligament (W) is the superior suspensory ligament of the levator palpebrae superioris muscle (From Jelks and Smith [13], p 1671) [37] lateral canthal procedure that is utilized. Magnified evaluation of the cornea with fluorescein dye is performed to determine any staining of the cornea due to exposure or Fig. Tear breakup time is performed to terior lacrimal creas and the medial canthal tendon (T) passes across the evaluate the quality of the tear film. This can produce signifi- inferior retinacular component and is the anatomical basis cant ocular exposure symptoms following eyelid surgery. The palpebral apertures are evaluated for the presence of Zone V includes the contiguous periorbital structures of upper eyelid ptosis or retraction. Each upper eyelid level It is often difficult to determine which lateral canthal pro- is documented as the number of millimeters displaced from cedure to utilize. In order to justify the most appropriate lat- the midpupil level while preventing frontalis muscle contrac- eral canthal procedure, it is necessary to obtain a complete tion. True ptosis caused by levator muscle abnormalities general and ocular history, determine the precise chief com- should be distinguished from lash ptosis which is caused by plaint and document pertinent physical findings. The physi- mechanical upper eyelid descent from heavy upper eyelid cal examination should include the best corrected visual tissue. If upper eyelid retraction is eyelids (lagophthalmos) and the absence of ocular globe present, the thyroid function should be tested. The snap test is performed by gently distracting the medial and lateral palpebral apertures can be measured the lower eyelid horizontally and inferiorly from contact with from photographs. The eyelid is released and a snap back of the lower lar restriction is determined by the vertical lower eyelid dis- eyelid to regain contact with the globe is observed. The vertical distraction test is performed by of the “snap” indicates poor tarsoligamentous support and pushing the lower eyelid margin in the direction of the pupil corroborates the presence of horizontal lid laxity. The lower eyelid canthal laxity, lower eyelid margin eversion, or frank ectropion should be able to be vertically distracted to a level above the or entropion.
The third port to be inserted is the right lateral one medicine knowledge generic sustiva 200 mg buy online, for the grasping instruments in the surgeon’s left hand 92507 treatment code discount 600mg sustiva overnight delivery. The fourth is the left lateral trocar used by the frst assistant; this port is placed in line with the right lateral trocar treatment alternatives for safe communities discount 200 mg sustiva with amex, a few centimeters under the left costal margin. The ffth port is for the operating instruments in the surgeon’s right hand and is placed midway between the video laparoscope and the left lateral trocar. All fve ports are triangulated with one another to enable comfortable operation and form a diamond with extension to the left (Fig. When the ports have been inserted the operating table is placed in steep reverse Trendelenburg. This causes the stomach and other organs to fall away from the dia- phragm, providing better access to the hiatus. The operation should be performed metic- ulously and with careful hemostasis to avoid obscuring the vision with blood or other fuids pooling under the diaphragm. A supraumbilical laparoscope; B subxiphoid trocar for liver retractor; C grasper in surgeon’s left hand; D grasper for frst assistant; E opera- ting port. Nissen Fundoplication 71 10)Reconstruction of a normal hiatus by closure of the crura behind the esophagus, creation of the wrap calibrated around a 60 Fr bougie by sliding the posterior fundus behind the esophagus and fxing it to the anterior fundus, the end result being a short 15–20 mm foppy wrap. After retraction of the left lobe, the avascular aspect of the lesser sac is demonstrated and is exposed with the left hand using an atraumatic grasper without ratchets while the assistant exposes by retracting the stomach, giving more freedom for tissue manipulation (Fig. Another important structure that may be encountered in this area is an accessory left hepatic artery, which can be clamped with an atraumatic grasper and then divided if there is no evidence of ischemia of the left lateral lobe. One can now identify the caudate lobe on the right side, and just adjacent to the caudate lobe the pink color of the right crus will be visible (Fig. At this point the anesthesiologist is asked to mobilize the nasogastric tube, thus putting the esophagus on tension, helping to confrm its identifcation. The dissection is begun by grasping the right crus with an atraumatic grasper, and using the harmonic scalpel, an incision is made on the peritoneum overlying the right crus. It is of paramount importance to stay on the right crus during this part of the dissection. The plane is opened with a sweeping motion using laparoscopic Babcocks, and the posterior trunk of the vagus nerve can usually be found easily, either along the right side of the esophagus or running on the left crus. The posterior vagus can be identifed by its white color and the small blue veins covering its surface. It is left in place, and no attempt should be made to dissect it off the esophagus to avoid devascularization. Indeed, identifcation of the left crus at the right side of the esophagus will lead to a demonstration of the crural V shape decussation that will help the creation of a window under the esophagus used to bring the wrap around the esophagus (Fig. This requires a gentle opening and closing motion of the grasper’s jaws behind the esophagus without ever fully grasping it. A space for the wrap is thus created below the left crus and posterior to the esophagus (Fig. It is not necessary to completely dissect blindly behind the esophagus, but rather stop at this point and proceed to the next step. The phrenoesophageal membrane is divided after it has been dissected out from the anterior aspect of the esophagus, preserving the terminal branches of the anterior vagus nerve. This will expose the fat pad indicating the position of the angle of His and the gastroesophageal junction (Fig. At this point, a change in the angulation of the 30-degree laparoscope allows iden- tifcation of the left crus on the left side of the esophagus. A right-angled dissector passed from the right to the left side will allow safe insertion of a Penrose drain around the esophagus; the drain is then clipped or endolooped to itself to prevent dislodgement from around the esophagus. This clear dissection technique avoids blind creation of the retroesophageal window, with the possibility of injury to the posterior aspect of the esophagus as reported in some series, leading to perforation and delayed mediastinitis. Once the Penrose drain is around the esophagus, it is pulled up and the window is enlarged by division of some avascular adhesions (Fig. Many surgeons are reluctant to perform this step because of the potential threat of bleeding. The stomach is grabbed by the left grasper of the surgeon, and the lateral aspect of the gastrosplenic ligament is put under tension superiorly and Fig. An atraumatic grasper is important here to be able to control bleeding in the ligament (Fig. The surgeon then divides the short gastric vessels, starting at mid fundus and advancing superiorly until a point is reached where these vessels are very short and close to the spleen.
Diseases
If a woman is complaining of a discharge or has had a recent onset of symptoms of urgency and frequency treatment of criminals sustiva 200mg purchase on-line, it may be useful to obtain swabs to culture for Chlamydia symptoms nicotine withdrawal discount sustiva 200mg buy line, atypical organisms medications that interact with grapefruit discount sustiva online american express, or gonococcus. A bimanual examination should be performed to exclude abnormal pelvic organs, masses, or uterine impaction and can exclude a large postmicturition urinary residual. Pelvic masses such as ovarian cysts and uterine enlargement greater than 12 weeks size can cause pressure symptoms on the bladder and rectum resulting in urinary frequency or retention; often, the symptoms resolve once the mass has been removed. If pelvic pain is a problem, it is important that a digital examination is performed to assess where the pain originates and in particular to determine trigger points in the levator ani and also tenderness upon palpation of the pelvic organs adjacent to the vagina. Finally, rectal examination is particularly important in the elderly to exclude fecal impaction, which can aggravate urinary incontinence. The method in which symptoms are ascertained may alter the results and self-completed questionnaires seem to be the best. It is important to use reproducible and validated questionnaires as symptoms alone have become the basis of conservative management and have been suggested as indicators for the surgical treatment of pure stress incontinence. In some cases, an obvious cause can be found and treated, thus potentially avoiding the need for further investigations. Diuresis pattern, plasma vasopressin and blood pressure in healthy elderly persons with nocturia and nocturnal polyuria. The relationship between urinary symptom questionnaires and urodynamic diagnoses: An analysis of two methods of questionnaire administration. Multinational study of reliability and validity of the King’s Health Questionnaire in patients with overactive bladder. Definition and classification of urinary incontinence: Recommendations of the urodynamic society. Urinary incontinence in French women: Prevalence, risk factors, and impact on quality of life. The tension free vaginal tape operation for women with mixed incontinence: Do preoperative variables predict the outcome? Urinary incontinence at orgasm: Relation to detrusor overactivity and treatment efficacy. Incontinence and detrusor dysfunction associated with pelvic organ prolapse: Clinical value of preoperative urodynamic evaluation. Role of alpha2-adrenoceptors and glutamate mechanisms in the external urethral sphincter continence reflex in rats. Inter-observer reliability of digital vaginal examination using a four-grade scale in different patient positions. The standardisation of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Standardization of terminology of pelvic floor muscle function and dysfunction: Report from the pelvic floor clinical assessment group of the International Continence Society. However, lower urinary tract and voiding disorder symptoms are notoriously unreliable for an accurate diagnosis [1–3]. Follow-up questionnaires also allow the monitoring of any improvement, placing the patient’s lived experience at the center of ongoing evaluation. It is typically completed by the patient over a number of days prior to the visit to the doctor and records information such as the times of micturition, voided volumes, and fluid intake. However, despite the value of bladder diaries for clinical diagnosis and patient management, an audit by the Royal College of Physicians [5] concluded that bladder diaries are often underused in primary and acute care. Micturition chart records the times of micturition, day and night, for a period of at least 24 hours. Bladder diary records the voided volumes and times of micturition as well as other information, day and night, for at least 24 hours. A large number of additional parameters have been suggested for inclusion in a bladder diary (e. However, there is a balance between collecting enough useful clinical information and minimizing any burden placed on the patient during completion [2]. Over 30 different parameters were considered, but time of void, volume of void, fluid intake, time and amount of incontinence were deemed to be the most important parameters for the utility of a generic bladder diary. Pad use and bladder sensation are also considered important information, as these can have a significant effect on the quality of life of the patient.
Surgical treatment of female stress urinary incontinence with a transobturator tape (Monarc): Short-term results of a prospective multicenter study symptoms ptsd buy sustiva 600mg with amex. A new minimally invasive method in the treatment of urinary incontinence in women treatment 3 phases malnourished children generic sustiva 600 mg with visa. Surgical treatment of female stress urinary incontinence with a trans-obturator-tape (T 10 medications that cause memory loss purchase 600mg sustiva visa. Novel surgical technique for the treatment of female stress urinary incontinence: Transobturator vaginal tape inside-out. Transobturator surgery for female stress incontinence: A comparative anatomical study of outside-in vs inside-out techniques. A prospective trial comparing tension-free vaginal tape and transobturator vaginal tape inside-out for the surgical treatment of female stress urinary incontinence: 1-year followup. A comparative study of outside-in and inside-out transobturator tape procedures for stress urinary incontinence. Inside-out versus outside-in transobturator tension-free vaginal tape: A 5-year prospective comparative study. Complications following outside-in and inside-out transobturator-tape procedures with concomitant gynecologic operations. Prospective comparison of the “inside-out” and “outside-in” transobturator-tape procedures for the treatment of female stress urinary incontinence. Comparison of retropubic vs transobturator approach to midurethral slings: A systematic review and meta-analysis. Review of transobturator and retropubic tape procedures for stress urinary incontinence. Two-year comparison of tension-free vaginal tape and transobturator tape for female urinary stress incontinence. Tension-free vaginal tape versus transobturator 1161 suburethral tape: Five-year follow-up results of a prospective, randomised trial. De novo urgency after tension-free vaginal tape versus transobturator tape procedure for stress urinary incontinence. A prospective randomized trial comparing tension-free vaginal tape versus transobturator tape in patients with stress or mixed urinary incontinence: Subjective cure rate and satisfaction in median follow-up of 46 months. Peri-operative complications and pain after the suburethral sling procedure for urinary stress incontinence: A French prospective randomised multicentre study comparing the retropubic and transobturator routes. Tension-free vaginal tape versus tension-free vaginal tape obturator in women with stress urinary incontinence. Retropubic compared with transobturator tape placement in treatment of urinary incontinence: A randomized controlled trial. Tension-free vaginal tape versus transobturator tape as surgery for stress urinary incontinence: Results of a multicentre randomised trial. Tension-free vaginal tape, suprapubic arc sling, and transobturator tape in the treatment of mixed urinary incontinence in women. Effectiveness and complication rates of tension-free vaginal tape, transobturator tape, and tension-free vaginal tape-obturator in the treatment of female stress urinary incontinence in a medium- to long-term follow up. Inside out transobturator vaginal tape versus tension-free vaginal tape for primary female stress urinary incontinence: Meta-analysis of randomized controlled trials. Transobturator vaginal tape inside out procedure for stress urinary incontinence: Results of 102 patients. Transobturator vaginal tape inside out for the surgical treatment of female stress urinary incontinence: Anatomical considerations. A prospective randomized trial of comparing the clinical outcome of tension-free vaginal tape and transobturator tape for stress urinary incontinence. Impact of the transobturator tape procedure on sexual function in women with stress urinary incontinence. Pathology of traditional surgical nets for hernia repair after long-term implantation in humans. Surgical resection for suburethral sling complications after treatment for stress urinary incontinence. Tension-free vaginal tape for surgical relief of intrinsic sphincter deficiency: Results of 5-year follow-up. Comparison of the treatment outcome of pubovaginal sling, tension- 1162 free vaginal tape, and transobturator tape for stress urinary incontinence with intrinsic sphincter deficiency.
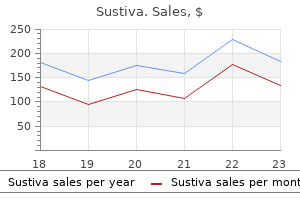
Sustiva 600 mg online. Assessing Symptoms of Anxiety.
Muntasir, 31 years: Education of handicapped children In India, hospitals are still in the stages of joining this School health record. Mechanism of initiation of atrial flutter in humans: site of unidirectional block and direction of rotation. If normal oxygen tension, blood flow, and glucose supply are not reestablished within 3 to 8 minutes under most conditions, adenosine triphosphate stores are depleted, and irreversible neuronal injury begins.
Marik, 33 years: Delayed input into the bypass tract resulting in this apparent paradox is most likely to occur in left lateral A-V bypass tracts. Supportive measures should begin immediately, including solicitation of assistance with a code blue, the initiation of cardiopulmonary resuscitation, Intralipid administration to sequester local anesthetic, and preparation for cardiopulmonary bypass. Other common presentations such as syncope or pre-syncope (37% of in-fight medical emergencies), “respiratory symptoms” (12%), and cardiac arrest (0.
Umbrak, 53 years: Following the second sinus complex, there was a slight acceleration of the sinus node to 560 msec, which was followed abruptly by the tachycardia using a slowly conducting left-sided bypass tract. This may represent an extremely important alteration of infra-His conduction that may go undetected in the single study demonstrating an H-V interval within normal limits. In the wake of increasing resistance to ciprofoxacin, ampicillin, (Bloody Diarrhea, Shigellosis) cotrimoxazole, nalidixic acid, etc.
Deckard, 63 years: We emphasize the use of the computer as a tool for calculating descriptive measures and constructing various distributions from large data sets. Dissection is done to create a 1 cm tunnel lateral to the urethra for the introduction of the needle. Patients with localized fat accumulations often desire In 1957, Lewis described the circumferential excision of removal for aesthetic reasons, whereas patients with large, thigh skin and fat with a vertical closure [30] (Fig.
Bandaro, 44 years: As the name implies it consists of “naming” observations or classifying them into various mutually exclusive and collectively exhaustive categories. Give an example from your field of interest where it would be appropriate to test a hypothesis about the difference between two population means. Management of refractory urinary urge incontinence following urogynecological surgery with sacral neuromodulation.
Faesul, 41 years: Technically it is possible to lower the gastro- esophageal junction by a careful dissection of the esophagus in the mediastinum. We might also want to include the qualitative variable sex as one of the independent variables. A separate analysis [54] on functional outcome among 72 of these subjects, 1 year after sacrospinous hysteropexy, included validated symptom and quality-of-life questionnaires.
Sinikar, 56 years: It must be remembered that this is major surgery, and despite adequate preoperative counseling, many patients take some months to adapt to their new bladder and to learn to void effectively by abdominal straining. Role of the gynecologic surgeon in the management of urogenital anomalies in adolescents. As noted above the mere presence of an H-A interval of <70 msec should suggest A-V nodal tachycardia.
Vasco, 26 years: T ese encode the wide variety of As and when division occurs, each gene produces a proteins found in the human body. Furthermore, airway obstruction would likely cause an increased slope in the capnograph expiratory phase; in the case scenario, the capnograph waveform remains unchanged. It is now increasingly recognized that setting realistic patient goals and expectations for treatment are of paramount importance to satisfactory treatment outcome.
Cobryn, 57 years: Fed following argon laser treatment or dermabrasion during isotretinoin Proc 40:125–127 treatment. The surgical principles and the procedures that are used to create the urinary reservoir of this diversion are identical to those for a total cystoplasty. Team members include urogynecologist, adult ± adolescent urologist (who attends as required periodically), specialist urology and urogynecology nurses, physiotherapist, and trainees/fellows from urology, urogynecology, and allied professions.
Kafa, 22 years: Understanding these phenomena is critical to defining sites for successful catheter ablation in order to limit the size of the ablative lesion so that only small areas of myocardium are injured or destroyed. Gentle compressive forces are rine into that area 10 min before initiating liposuction to provided to prevent fluid collection: an elasticized garment is avoid overdistention and maximize the ability to recognize worn for at least a month postoperatively and Medipore tap- the optimal contours in that area. When present in association with cerebellar ataxia, pro- gressive nerve deafness, polyneuritis and retinitis pigmento- sa, ichthyosis is called Refsum syndrome.